A 42-year-old Indian man presents with a 3-month history of progressive abdominal distension and early satiety. On examination, he has massive splenomegaly and mild hepatomegaly. Laboratory investigations reveal hemoglobin 9.2 g/dL, WBC 68,000/μL with 60% lymphocytes, and platelets 95,000/μL. Peripheral blood smear shows small, mature-appearing lymphocytes with scant cytoplasm. Bone marrow biopsy shows nodular infiltration of small lymphocytes. Flow cytometry reveals CD5+, CD19+, CD23+ B cells. What is the most likely diagnosis?
A. Follicular lymphoma
B. Marginal zone lymphoma
C. Chronic lymphocytic leukemia / Small lymphocytic lymphoma
D. Lymphoplasmacytic lymphoma
Explanation
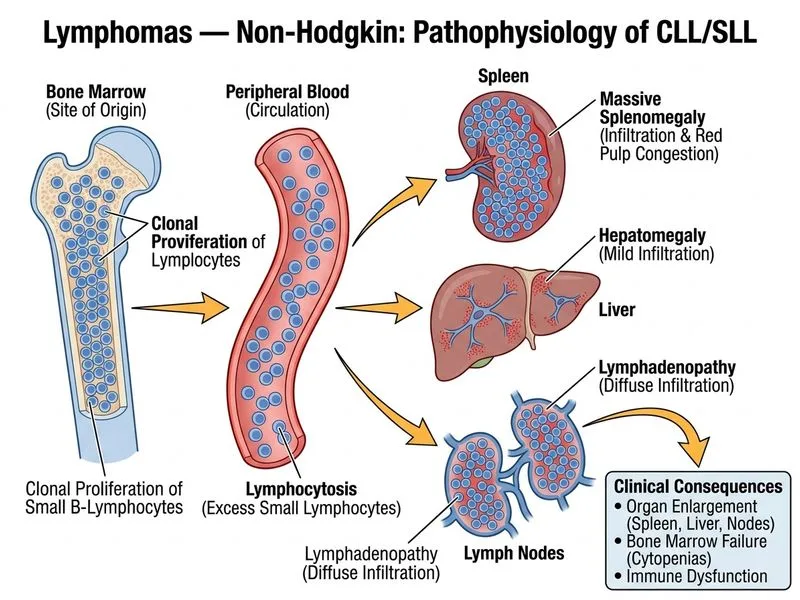
Diagnosis: Chronic Lymphocytic Leukemia / Small Lymphocytic Lymphoma (CLL/SLL)
Clinical Presentation
The patient presents with:
Insidious onset (3 months) of abdominal symptoms
Massive splenomegaly and hepatomegaly
Cytopenias (anemia, thrombocytopenia)
Marked lymphocytosis (68,000/μL) with mature small lymphocytes
Key Point
CLL/SLL is the most common B-cell lymphoma in Western countries and increasingly in India. It typically affects middle-aged to elderly patients and often presents with lymphocytosis discovered incidentally or with cytopenias.
Immunophenotype — The Diagnostic Hallmark
Table
Feature
CLL/SLL
Follicular
Marginal Zone
Lymphoplasmacytic
CD5
Positive
Negative
Negative
Negative
CD19
Positive
Positive
Positive
Positive
CD23
Positive
Negative
Variable
Negative
Surface Ig
Weak
Strong
Strong
Strong
Cytology
Small, mature
Centrocytes, centroblasts
Small lymphocytes, monocytoid cells
Small lymphocytes, plasma cells
High-YieldNEET PG
The CD5+, CD19+, CD23+ phenotype is virtually pathognomonic for CLL/SLL. CD5 is a T-cell marker aberrantly expressed on B cells in CLL — this is the "coexpression" that clinches the diagnosis.
Morphology & Bone Marrow
Small, mature lymphocytes with scant cytoplasm and clumped chromatin ("soccer ball" nuclei)
Nodular or diffuse infiltration of bone marrow
Smudge cells (fragile lymphocytes) often seen on blood smear
Clinical Pearl
Massive splenomegaly in CLL suggests advanced disease (Rai stage III–IV or Binet stage C). The combination of lymphocytosis + organomegaly + cytopenias is classic for CLL.
Why This Is CLL/SLL and Not Other Indolent Lymphomas
Follicular lymphoma would show:
CD5−, CD10+, BCL2+ (t(14;18))
Centrocytes and centroblasts in germinal center pattern
Typically nodal presentation, not massive splenomegaly
Marginal zone lymphoma would show:
CD5−, CD23− (or weakly positive)
Monocytoid B cells in marginal zone pattern
Often associated with Sjögren's syndrome or hepatitis C
Lymphoplasmacytic lymphoma would show:
CD5−, CD23−
Admixture of small lymphocytes and plasma cells
Often associated with Waldenström macroglobulinemia (monoclonal IgM)
Mnemonic
CD5-CD23 Co-Expression = CLL — Remember: "CLL has CD5 and CD23."
Staging & Prognosis
This patient has:
Rai stage III (anemia, organomegaly) or Binet stage C (lymphocytosis + organomegaly + anemia)
Intermediate to poor prognosis
Requires monitoring for Richter transformation (10–15% risk) and autoimmune complications
High-YieldNEET PG
CLL/SLL is incurable with conventional chemotherapy but has improved survival with targeted agents (BTK inhibitors like ibrutinib, anti-CD20 monoclonal antibodies like rituximab).
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.