## Diagnosis: Pernicious Anemia (Cobalamin Deficiency) ### Clinical Presentation **Key Point:** The constellation of glossitis, paresthesias (peripheral neuropathy), and pancytopenia with megaloblastic anemia in a vegetarian patient points to vitamin B12 deficiency. ### Laboratory Findings | Finding | Significance | |---------|-------------| | MCV 112 fL | Macrocytic anemia (>100 fL) | | Hypersegmented neutrophils | Nuclear maturation lag — hallmark of megaloblastosis | | Macro-ovalocytes | Immature RBC release due to nuclear-cytoplasmic asynchrony | | Serum B12 145 pg/mL | Diagnostic threshold; <200 pg/mL confirms deficiency | | Low reticulocyte count (0.8%) | Ineffective erythropoiesis; marrow cannot compensate | | Pancytopenia | Affects all cell lines due to impaired DNA synthesis | **High-Yield:** Pernicious anemia is autoimmune destruction of gastric parietal cells → loss of intrinsic factor → B12 malabsorption. In this vegetarian patient, dietary B12 deficiency is the mechanism. ### Pathophysiology of Megaloblastosis 1. B12 is a cofactor for methylmalonyl-CoA mutase and methionine synthase 2. B12 deficiency → impaired thymidylate synthesis → defective DNA replication 3. Nuclear maturation lags behind cytoplasmic maturation → asynchronous development 4. Hypersegmented neutrophils (>5 lobes) and macro-ovalocytes result 5. Ineffective erythropoiesis → low reticulocyte count despite anemia **Clinical Pearl:** The presence of neurological symptoms (paresthesias, vibration sense loss) is pathognomonic for B12 deficiency and distinguishes it from folate deficiency — folate deficiency does NOT cause neuropathy. **Mnemonic: B12 NEURO** — B12 deficiency causes Neuropathy, Encephalopathy, Reversible (if caught early) dementia, Optic atrophy, Subacute combined degeneration. ### Why B12 Deficiency, Not Folate? - Folate deficiency also causes megaloblastic anemia and pancytopenia - **BUT:** Folate deficiency does NOT cause neurological symptoms (no neuropathy, no subacute combined degeneration) - This patient has clear neurological findings → B12 deficiency is diagnostic - Serum B12 is low; folate level would be normal in pure B12 deficiency [cite:Robbins 10e Ch 14] 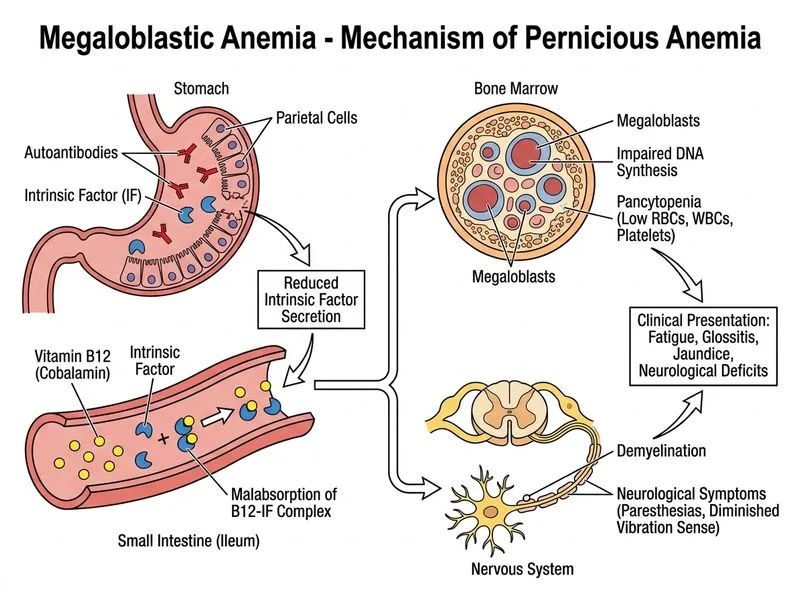
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.