## Diagnosis: Combined Megaloblastic Anemia (B12 + Folate Deficiency) ### Clinical Context: Celiac Disease **Key Point:** Celiac disease causes villous atrophy and malabsorption of multiple nutrients, including both cobalamin (terminal ileum) and folate (proximal small intestine). This patient has BOTH deficiencies. ### Laboratory Evidence of Dual Deficiency | Parameter | Finding | Interpretation | |-----------|---------|----------------| | MCV | 104 fL | Macrocytic anemia | | Serum B12 | 180 pg/mL | Low (normal >200) | | Serum folate | 2.2 ng/mL | Low (normal >5.4) | | Hypersegmented neutrophils | Present | Megaloblastosis | | Macro-ovalocytes | Present | Nuclear-cytoplasmic asynchrony | | Giant metamyelocytes | Present on BM | Severe megaloblastic changes | | Pancytopenia | WBC 3200, plt 110K | Affects all cell lines | **High-Yield:** In celiac disease, both B12 and folate are malabsorbed. However, the **neurological symptoms** (forgetfulness, paresthesias) are pathognomonic for B12 deficiency — folate deficiency alone does NOT cause neuropathy. ### Pathophysiology 1. **Folate deficiency** → impaired thymidylate synthesis → megaloblastic anemia, pancytopenia 2. **B12 deficiency** → impaired methionine synthase → methylation defects → neurological damage (subacute combined degeneration, cognitive changes) 3. Both contribute to the anemia; B12 is responsible for neurological manifestations ```mermaid flowchart TD A[Celiac Disease: Villous Atrophy]:::outcome --> B[Malabsorption of Multiple Nutrients] B --> C[Folate Deficiency<br/>Proximal SI]:::outcome B --> D[B12 Deficiency<br/>Terminal Ileum]:::outcome C --> E[Impaired DNA Synthesis]:::action D --> F[Impaired Methylation]:::action E --> G[Megaloblastic Anemia<br/>Pancytopenia]:::outcome F --> H[Neurological Damage<br/>Cognitive decline, Neuropathy]:::urgent G --> I[Combined Megaloblastosis]:::outcome H --> I ``` **Clinical Pearl:** When a patient with megaloblastic anemia has BOTH low B12 and low folate, the neurological findings (if present) indicate that B12 deficiency is the primary driver of the neurological component. Treating folate alone without B12 can mask B12 deficiency and allow neurological damage to progress ("folate trap"). **Mnemonic: FOLATE TRAP** — Folate supplementation without B12 correction can mask B12 deficiency; hematologic improvement occurs (folate corrects DNA synthesis), but neurological damage continues unchecked. ### Why This Is Combined Deficiency - Both serum B12 AND serum folate are low - Both are malabsorbed in celiac disease - Neurological symptoms (forgetfulness, paresthesias) point to B12 as the primary neurological culprit - Bone marrow shows severe megaloblastosis consistent with both deficiencies [cite:Robbins 10e Ch 14; Harrison 21e Ch 98] 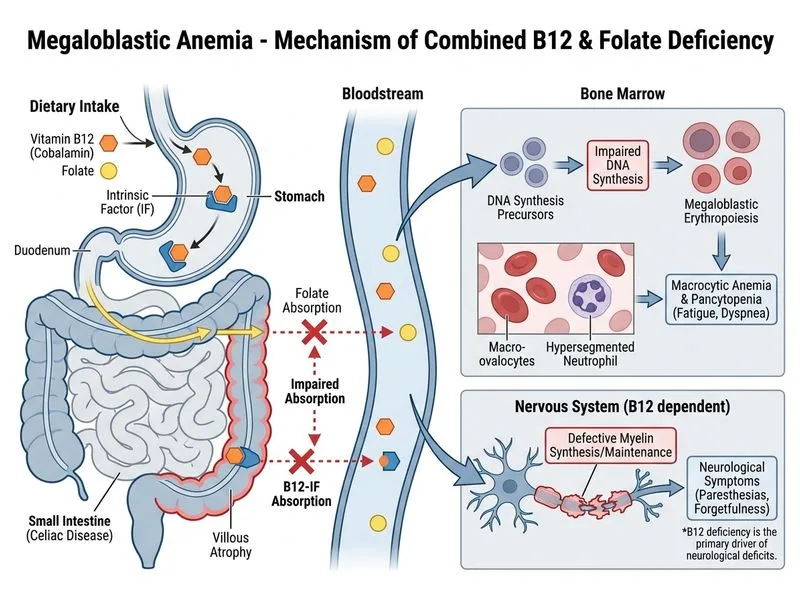
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.