## Acute Decompensation in Chronic Megaloblastic Anemia: Dual Pathology ### Clinical Scenario Analysis **Key Point:** This patient has two simultaneous processes: 1. **Worsening megaloblastic anemia** (baseline B12 deficiency with acute drop in Hb) 2. **Superimposed autoimmune hemolytic anemia (AIHA)** — evidenced by hemolysis markers ### Evidence for Hemolysis | Marker | Finding | Interpretation | |--------|---------|----------------| | **Reticulocyte count** | 8.2% | Markedly elevated (normal <2%), indicating compensatory erythropoiesis | | **LDH** | 1200 U/L | Significantly elevated (RBC destruction releases LDH) | | **Indirect bilirubin** | 3.2 mg/dL | Elevated (unconjugated hyperbilirubinemia from hemolysis) | | **Haptoglobin** | <10 mg/dL | Severely depleted (consumed by binding free hemoglobin) | | **Icterus** | Present | Clinical sign of hyperbilirubinemia | | **Splenomegaly** | Present | Extramedullary hemolysis and erythrophagocytosis | **High-Yield:** The combination of elevated reticulocyte count (8.2%) + elevated LDH + low haptoglobin + elevated indirect bilirubin is the **diagnostic triad of hemolysis**. ### Why This Is "Megaloblastic Crisis with Concurrent AIHA" **Clinical Pearl:** Patients with long-standing autoimmune conditions (including autoimmune gastric atrophy causing pernicious anemia) are at increased risk for developing secondary autoimmune hemolytic anemia. This patient likely developed AIHA superimposed on his chronic B12 deficiency. The acute drop in hemoglobin (8.5 → 6.2 g/dL) over 2 weeks, combined with hemolysis markers, indicates an acute hemolytic event layered on top of chronic megaloblastic anemia. ### Pathophysiology ```mermaid flowchart TD A[Chronic B12 Deficiency<br/>Pernicious Anemia]:::outcome --> B[Baseline Hb 8.5 g/dL<br/>Megaloblastic changes]:::action A --> C[Autoimmune gastric atrophy<br/>Chronic autoimmune state]:::action C --> D[Secondary autoimmune<br/>hemolytic anemia develops]:::action D --> E[Acute hemolysis]:::urgent E --> F[Rapid drop in Hb<br/>Elevated reticulocytes<br/>Elevated LDH<br/>Low haptoglobin]:::outcome B --> G[Macrocytes<br/>Hypersegmented neutrophils<br/>Polychromasia on smear]:::outcome ``` ### Peripheral Blood Smear Interpretation **Key Point:** The smear shows BOTH megaloblastic features AND hemolytic features: - **Megaloblastic:** Macrocytes, hypersegmented neutrophils (from chronic B12 deficiency) - **Hemolytic:** Polychromasia (reticulocytes staining blue due to residual RNA), spherocytes (if AIHA is warm-antibody type) This dual pattern is pathognomonic for the combination diagnosis. ### Why Not Simple Folate Deficiency? **Warning:** Acute folate deficiency (e.g., from poor diet or increased demand) could worsen megaloblastic anemia, but it would NOT explain the hemolysis markers (elevated LDH, low haptoglobin, elevated indirect bilirubin, elevated reticulocytes). Folate deficiency causes ineffective erythropoiesis with LOW reticulocyte count, not the elevated reticulocyte count seen here. ### Management Implications **Clinical Pearl:** This patient requires: 1. **B12 supplementation** (continue/escalate) for pernicious anemia 2. **Corticosteroids** (prednisolone) for AIHA 3. **Possible IVIG or rituximab** if steroid-refractory 4. **Splenectomy** may be considered if medical therapy fails Treating only the B12 deficiency would fail to address the acute hemolytic component. [cite:Robbins and Cotran Pathologic Basis of Disease 10e Ch 14; Harrison's Principles of Internal Medicine 21e Ch 100 and Ch 139] 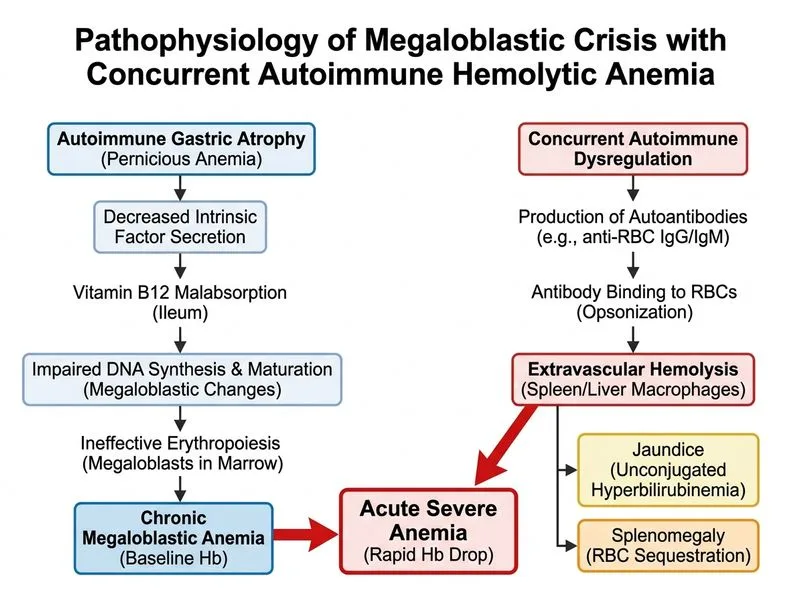
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.