## Clinical Diagnosis: MEN 1 Syndrome ### Key Clinical Features Present **Key Point:** MEN 1 is characterized by the "3 P's" — **P**arathyroid adenoma, **P**ancreatic neuroendocrine tumors, and **P**ituitary adenoma. This patient demonstrates the classic triad. ### Identifying Features in This Case | Feature | Finding | Significance | |---------|---------|---------------| | **Parathyroid involvement** | Elevated serum calcium (11.2 mg/dL) | Parathyroid adenoma/hyperplasia | | **Pancreatic tumor** | Gastrinoma (fasting gastrin 850 pg/mL) with refractory peptic ulcers | Gastrin-secreting neuroendocrine tumor (Zollinger-Ellison syndrome) | | **Thyroid nodule** | Palpable on exam | Thyroid involvement (adenoma or carcinoma) | | **Family history** | Son with parathyroid adenoma at age 22 | Autosomal dominant inheritance; early-onset suggests germline mutation | ### Pathophysiology **High-Yield:** MEN 1 results from inactivating mutations in the **MEN1 gene** (chromosome 11q13), which encodes menin — a tumor suppressor protein involved in transcriptional regulation and cell cycle control. Loss of menin function leads to: 1. Parathyroid hyperplasia → primary hyperparathyroidism (95% of MEN 1 patients) 2. Pancreatic/gastroenteropancreatic neuroendocrine tumors (60–70%) - Gastrinomas (most common functional tumor; causes Zollinger-Ellison syndrome) - Insulinomas - Non-functional tumors 3. Anterior pituitary adenomas (30–40%) - Prolactinoma (most common) - Growth hormone–secreting (acromegaly) - Non-functional 4. Other tumors: adrenocortical adenomas, thyroid adenomas, carcinoid tumors ### Diagnostic Criteria for MEN 1 **Key Point:** Diagnosis requires **≥2 of the 3 main tumors** OR **1 main tumor + a first-degree relative with MEN 1**. This patient has: - Parathyroid adenoma (elevated calcium) - Gastrinoma (elevated fasting gastrin, peptic ulcer disease) - Thyroid nodule - Positive family history (son with parathyroid adenoma) ### Why Not MEN 2A or 2B? **Mnemonic: MEN 2 = "C" for **C**alcitonin** — medullary thyroid carcinoma is the hallmark of MEN 2, not present here. - **MEN 2A:** Medullary thyroid carcinoma (MTC) + pheochromocytoma + parathyroid adenoma. No gastrinoma; no elevated gastrin. - **MEN 2B:** MTC + pheochromocytoma + mucosal neuromas + marfanoid habitus. No gastrinoma; no parathyroid involvement. This patient has **no evidence of MTC** (no calcitonin elevation, no medullary carcinoma on imaging) and **no pheochromocytoma** (though hypertension is present, it is likely secondary to hypercalcemia). ### Management Implications **Clinical Pearl:** MEN 1 requires lifelong surveillance: - Annual biochemical screening (serum calcium, prolactin, fasting gastrin, insulin, glucose) - Periodic imaging (MRI pancreas/pituitary, thyroid ultrasound) - Genetic counseling and testing of first-degree relatives - Early intervention to prevent complications (peptic ulcer perforation, hypercalcemic crisis, pituitary apoplexy) [cite:Robbins 10e Ch 24] 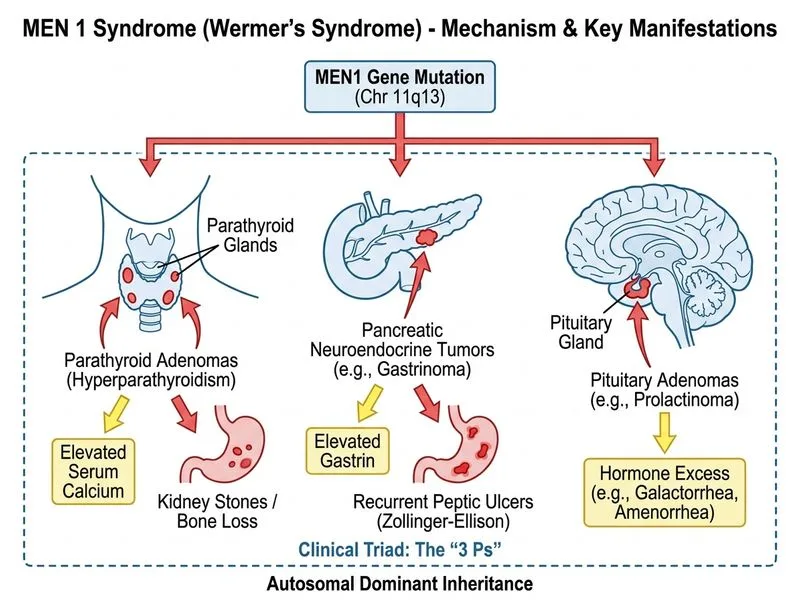
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.