## Diagnosis: MEN 1 Syndrome ### Clinical Presentation Analysis This patient presents with the classic triad of MEN 1: 1. **Primary hyperparathyroidism** — hypercalcemia (11.8 mg/dL), elevated PTH (185 pg/mL), and nephrolithiasis 2. **Pituitary adenoma** — growth hormone-secreting adenoma in his son (familial clustering) 3. **Pancreatic neuroendocrine tumor** — implied by the constellation of findings in a family member **Key Point:** MEN 1 is an autosomal dominant syndrome caused by mutations in the *MEN1* gene (chromosome 11q13), encoding menin protein. The "3 P's" mnemonic helps recall the main tumors: **Parathyroid**, **Pancreatic**, and **Pituitary** adenomas. ### Why This Is MEN 1, Not MEN 2A | Feature | MEN 1 | MEN 2A | |---------|-------|--------| | **Primary tumor** | Parathyroid adenoma (95%) | Medullary thyroid carcinoma (100%) | | **Pituitary involvement** | Prolactinoma, GH-secreting (common) | Rare | | **Pancreatic NETs** | Common (60–70%) | Absent | | **Medullary thyroid cancer** | Absent | Present (always) | | **Pheochromocytoma** | Absent | Present (50%) | | **Gene mutation** | *MEN1* | *RET* proto-oncogene | **Clinical Pearl:** MEN 2A would present with medullary thyroid carcinoma (often the first manifestation), pheochromocytoma, and parathyroid adenoma — but NOT with pituitary adenomas or pancreatic NETs. The presence of a GH-secreting pituitary adenoma in the family strongly favors MEN 1. ### Pathophysiology 1. Loss of menin (tumor suppressor) → loss of cell cycle control 2. Parathyroid hyperplasia/adenoma → PTH overproduction → hypercalcemia 3. Pancreatic islet cell adenomas → gastrinoma, insulinoma, non-functional tumors 4. Anterior pituitary adenomas → prolactin, GH, ACTH excess **High-Yield:** Screening in MEN 1 families includes: - Serum calcium, PTH, and 24-h urine calcium (parathyroid) - Fasting gastrin, insulin, glucose (pancreas) - Prolactin, IGF-1, ACTH levels (pituitary) - MRI pituitary and pancreas ### Management Implications - Genetic counseling and *MEN1* mutation testing - Screening of first-degree relatives (siblings, children) - Regular biochemical and imaging surveillance - Parathyroidectomy for symptomatic hyperparathyroidism - Monitoring for pancreatic NETs (especially gastrinoma) **Mnemonic:** **MEN 1 = "3 P's + Carcinoid"** - **P**arathyroid adenoma (95%) - **P**ancreatic NET (60–70%) - **P**ituitary adenoma (30–40%) - Plus: Adrenocortical tumors, carcinoid syndrome (thymic, bronchial, gastric) [cite:Robbins 10e Ch 24] 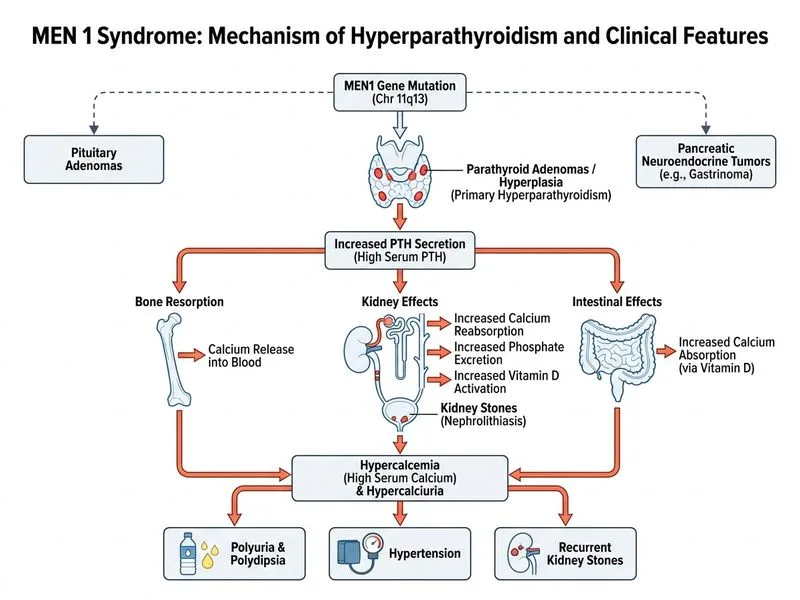
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.