## Diagnosis: MEN 2A Syndrome with Pheochromocytoma ### Clinical Presentation Breakdown This patient has the **classic triad of MEN 2A**: | Component | Finding | Significance | |-----------|---------|---------------| | **Medullary thyroid carcinoma (MTC)** | Diagnosed age 28; calcitonin 850 pg/mL | Earliest and most penetrant feature (100%) | | **Pheochromocytoma** | Hypertension, palpitations, sweating; elevated plasma metanephrines | Present in ~50% of MEN 2A | | **Primary hyperparathyroidism** | Calcium 10.8, PTH 78 (borderline elevated) | Present in ~20–30% of MEN 2A | | **RET codon 634 mutation** | Germline *RET* proto-oncogene | Diagnostic of MEN 2A (NOT MEN 2B) | **Key Point:** MEN 2A is caused by activating mutations in the *RET* proto-oncogene (chromosome 10q11.2). Codon 634 mutations are associated with the **highest risk of pheochromocytoma** (~50% penetrance) and are classified as **high-risk RET mutations** requiring prophylactic thyroidectomy by age 5–10 years in mutation carriers. ### Why NOT MEN 2B? **High-Yield:** MEN 2B is distinguished by: - Mucosal neuromas (lips, tongue, GI tract) — **absent in this patient** - Marfanoid habitus — **not mentioned** - Medullary thyroid carcinoma (earlier onset, more aggressive) - Pheochromocytoma (~50%) - **NO primary hyperparathyroidism** (key distinguishing feature) - *RET* mutations at codons 883, 918, or 922 (NOT codon 634) This patient has codon 634, which is **MEN 2A-specific**. ### Critical Management Principle: Pheochromocytoma First **Warning:** This is a high-yield exam trap. Many students proceed directly to thyroidectomy, but **pheochromocytoma must be treated BEFORE thyroid surgery** to prevent intraoperative hypertensive crisis and catecholamine surge. ```mermaid flowchart TD A[MEN 2A with MTC + Pheochromocytoma]:::outcome A --> B[Confirm pheochromocytoma diagnosis]:::action B --> C[Start alpha-blocker<br/>phenoxybenzamine 10 mg BD]:::action C --> D[Titrate to BP control<br/>then add beta-blocker]:::action D --> E[Imaging: CT/MRI abdomen<br/>MIBG scintigraphy]:::action E --> F{Surgical candidate?}:::decision F -->|Yes| G[Adrenalectomy]:::action F -->|No| H[Continued medical management]:::action G --> I[Then proceed to total thyroidectomy]:::action H --> I I --> J[Lifelong TSH suppression<br/>+ calcitonin monitoring]:::action ``` **Clinical Pearl:** Alpha-blockade MUST precede beta-blockade. Beta-blockers alone cause unopposed alpha-mediated vasoconstriction and hypertensive crisis. The sequence is: 1. **Alpha-blocker** (phenoxybenzamine 10 mg BD, titrate to 20–40 mg daily) — blocks catecholamine effects 2. **Beta-blocker** (propranolol, atenolol) — added only after alpha-blockade to control reflex tachycardia 3. **Imaging** (CT/MRI ± MIBG) — localize tumor 4. **Adrenalectomy** — definitive treatment 5. **Thyroidectomy** — after pheochromocytoma is controlled ### Why This Is NOT Option 3 (Sporadic) **High-Yield:** The germline *RET* mutation proves this is **hereditary MEN 2A**, not sporadic disease. Sporadic MTC and sporadic pheochromocytoma occurring together would be extremely rare and would NOT carry the same genetic implications for family screening. ### Why Option 4 Is Dangerous **Warning:** Starting a beta-blocker without alpha-blockade is contraindicated and can precipitate a hypertensive crisis. Beta-blockade alone leaves alpha-adrenergic effects unopposed, causing severe vasoconstriction and uncontrolled hypertension. ### Screening and Follow-up **Mnemonic:** **MEN 2A = "MTC + 2 others"** - **M**edullary **T**hyroid **C**arcinoma (100%) - **P**heochromocytoma (~50%) - **P**arathyroid adenoma (~20–30%) **High-Yield:** All first-degree relatives must undergo: - *RET* mutation testing - Plasma metanephrines (pheochromocytoma screening) - Serum calcium and PTH (parathyroid) - Calcitonin stimulation test (medullary thyroid) - Prophylactic thyroidectomy in childhood if mutation-positive [cite:Harrison 21e Ch 403; Robbins 10e Ch 24] 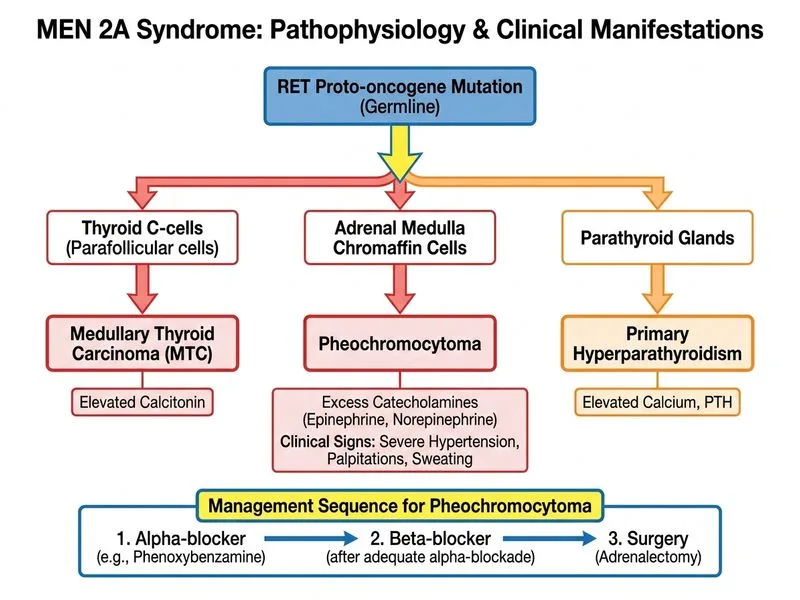
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.