A 62-year-old woman from Delhi presents with acute anterior wall myocardial infarction. She undergoes successful primary percutaneous coronary intervention (PCI) to the left anterior descending artery 90 minutes after symptom onset. Four days later, she develops acute decompensated heart failure with pulmonary edema. Echocardiography reveals a thin-walled, dyskinetic bulge in the anteroapical region of the left ventricle. Which of the following pathological processes is MOST likely responsible for the acute ventricular dysfunction at this 4-day timepoint?
A. Acute inflammatory infiltration with neutrophils and macrophages causing myocardial edema
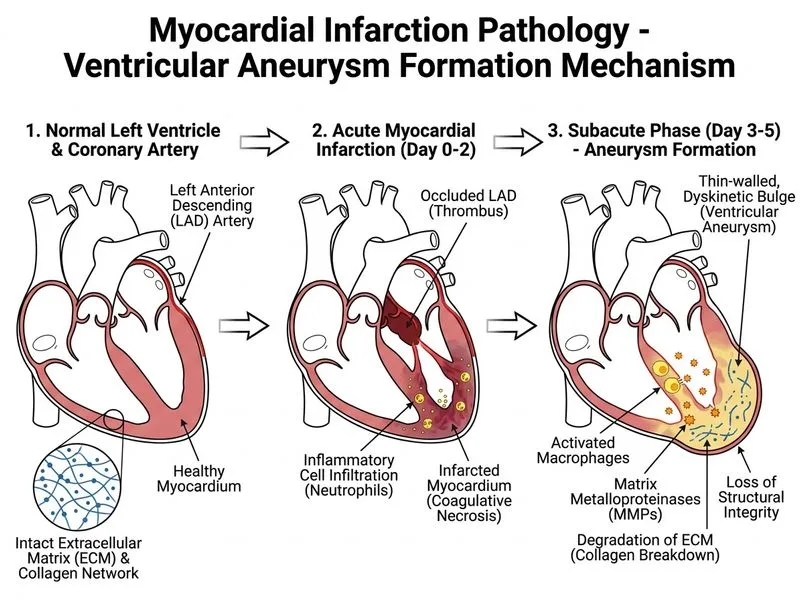
B. Loss of structural integrity due to degradation of the extracellular matrix by matrix metalloproteinases
C. Persistent myocardial stunning from prolonged ischemia-reperfusion injury
D. Collagen deposition and scar tissue formation replacing necrotic myocardium
Explanation
Post-Infarction Ventricular Rupture and Myocardial Wall Thinning
At 4 days post-MI, the infarcted myocardium is in a critical phase of structural vulnerability due to active inflammatory remodeling and enzymatic degradation of the extracellular matrix.
Matrix Metalloproteinases (MMPs) in Post-MI Remodeling
Key Point
At 4 days, the infarcted myocardium is undergoing active matrix degradation by matrix metalloproteinases (MMPs), particularly MMP-2 and MMP-9, which are released by infiltrating macrophages and neutrophils. This enzymatic breakdown of collagen and other extracellular matrix proteins weakens the wall and predisposes to rupture.
High-YieldNEET PG
The peak incidence of free wall rupture is 3–7 days post-MI, coinciding with maximum MMP activity and before collagen deposition provides structural support. At 4 days, the wall is thin and weak but not yet replaced by scar.
Clinical Pearl
The dyskinetic bulge (aneurysm) and acute decompensation at 4 days reflect loss of structural integrity from MMP-mediated matrix degradation, not from scar formation (which occurs later) or persistent stunning (which would improve with reperfusion).
Why Other Options Are Incorrect
Acute inflammatory infiltration (neutrophils/macrophages) causes edema but is not the primary driver of acute wall weakness at 4 days. Inflammation contributes to MMP activation but is not itself the mechanism of rupture risk.
Collagen deposition and scar formation are late changes (7–21 days) that stabilize the wall; at 4 days, collagen is being degraded, not deposited.
Myocardial stunning is a functional, reversible phenomenon that improves with reperfusion and time; it does not cause structural wall thinning or dyskinesia.
Mnemonic
MMP-4 — Matrix Metalloproteinases peak at day 4 (and days 3–7), causing Maximum wall Weakness and Myocardial rupture risk.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.