A 58-year-old man with a 2-day history of anterior wall myocardial infarction presents to the emergency department with acute dyspnoea, orthopnoea, and a new pansystolic murmur at the apex. Chest X-ray shows pulmonary oedema. Echocardiography reveals a ruptured papillary muscle with severe mitral regurgitation and an ejection fraction of 35%. What is the most appropriate immediate next step in management?
A. Start high-dose diuretics and ACE inhibitors; reassess in 48 hours
B. Administer intravenous dobutamine and observe for spontaneous stabilization
C. Perform immediate coronary angiography followed by percutaneous mitral valve repair
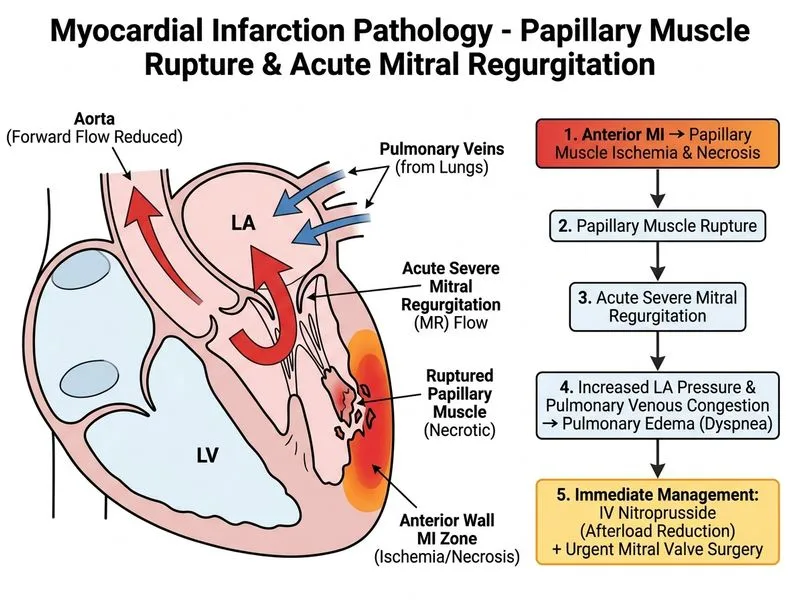
D. Initiate intravenous nitroprusside and arrange urgent cardiac surgery for mitral valve repair or replacement
Explanation
Clinical Context
This patient has acute mitral regurgitation secondary to papillary muscle rupture—a catastrophic mechanical complication of acute myocardial infarction occurring 2–7 days post-MI. The combination of acute dyspnoea, pulmonary oedema, and a new pansystolic murmur is pathognomonic.
Pathophysiology of Papillary Muscle Rupture
Key Point
Papillary muscle rupture occurs when transmural infarction extends into the base of the papillary muscle, causing necrosis and structural failure. The posteromedial papillary muscle (supplied by the RCA) is more commonly affected than the anterolateral papillary muscle.
Management Strategy
Immediate Stabilization
High-YieldNEET PG
Acute mitral regurgitation from papillary muscle rupture causes sudden volume overload and cardiogenic shock. Medical therapy alone is temporizing and insufficient.
1.
Reduce afterload with vasodilators (nitroprusside or nitroglycerin) to decrease regurgitant flow and improve forward cardiac output.
2.
Reduce preload with diuretics to relieve pulmonary congestion.
3.
Arrange urgent cardiac surgery — this is a surgical emergency. Mortality without surgery approaches 90% within 24 hours.
Why Surgery Is Mandatory
Clinical Pearl
Unlike other mechanical complications (e.g., small VSD), papillary muscle rupture cannot be managed medically or with percutaneous intervention. Surgical repair (suture of the ruptured papillary muscle head) or mitral valve replacement is the only definitive treatment.