## Opioid Rotation in Cancer Pain Management **Key Point:** Opioid rotation (switching to a different opioid at a reduced equianalgesic dose) is a well-established strategy for managing opioid-induced side effects and incomplete analgesia in cancer patients, particularly when dose escalation is limited by toxicity rather than inadequate pain control. ### Rationale for Opioid Rotation: - **Incomplete cross-tolerance:** Different opioids have varying receptor affinities, metabolite profiles, and pharmacokinetics. Switching to an alternative opioid at 25–30% dose reduction often improves analgesia while reducing side effects. - **Mechanism:** The patient's constipation and cognitive impairment suggest opioid toxicity; rotation exploits differences in metabolite accumulation (e.g., morphine-3-glucuronide vs. fentanyl's lack of active metabolites). - **Evidence:** Opioid rotation is recommended by WHO, ASCO, and NCCN guidelines for cancer pain management when dose escalation is limited by toxicity. ### Why Hydromorphone or Oxycodone? - Both are potent opioids suitable for severe cancer pain. - Hydromorphone has fewer active metabolites than morphine, potentially reducing cognitive side effects. - Oxycodone has intermediate metabolite profile and good oral bioavailability. **Clinical Pearl:** The 25–30% dose reduction accounts for incomplete cross-tolerance and reduces the risk of overdose while maintaining or improving analgesia. ### Multimodal Approach: While the correct answer focuses on opioid rotation, adjuvant agents (gabapentin, regional blocks) may be added concurrently but are not the primary intervention here. 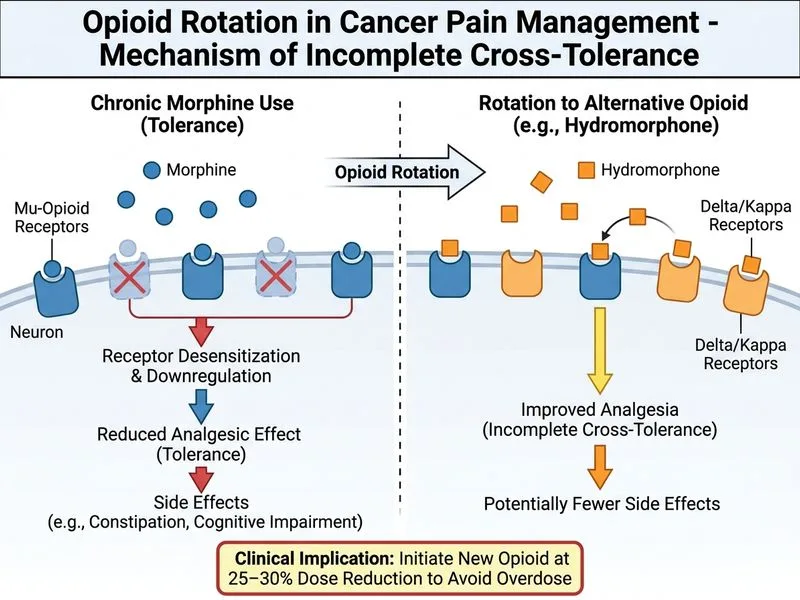
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.