## Lambert-Eaton Myasthenic Syndrome (LEMS) ### Definition Lambert-Eaton myasthenic syndrome (LEMS) is a paraneoplastic neuromuscular disorder caused by autoimmune attack on presynaptic voltage-gated calcium channels (VGCC), particularly P/Q-type channels. ### Pathophysiology 1. Malignant cells express calcium channel antigens 2. Immune system generates antibodies against P/Q-type VGCC 3. Antibodies bind to presynaptic terminals at neuromuscular junction 4. Reduced calcium influx → decreased acetylcholine release 5. Clinical result: muscle weakness and autonomic dysfunction ### Association with Small Cell Lung Cancer **Key Point:** SCLC is the most common malignancy associated with LEMS, occurring in 50–60% of LEMS patients. LEMS is present in 2–3% of SCLC patients. **High-Yield:** LEMS is a hallmark paraneoplastic syndrome of SCLC and should prompt immediate malignancy screening if not already diagnosed. ### Clinical Features | Feature | Characteristic | |---------|----------------| | Muscle weakness | Proximal > distal; legs > arms; improves with activity ("warm-up" phenomenon) | | Autonomic dysfunction | Dry mouth, impotence, constipation, reduced sweating | | Reflexes | Absent or diminished (areflexia) | | Fatigue | Prominent | | Respiratory involvement | Less common than in myasthenia gravis | ### Diagnostic Findings - **Serology:** Anti-P/Q-type VGCC antibodies (positive in ~85% of LEMS) - **Electromyography (EMG):** Low-amplitude compound muscle action potentials (CMAPs) with post-tetanic potentiation - **Repetitive nerve stimulation:** Decremental response at low frequencies; incremental response at high frequencies (opposite of myasthenia gravis) **Mnemonic:** LEMS = **L**ow amplitude, **E**xercise improves, **M**uscle weakness, **S**mall cell lung cancer ### Distinction from Myasthenia Gravis | Feature | LEMS | Myasthenia Gravis | |---------|------|-------------------| | Weakness pattern | Proximal > distal | Ocular > generalized | | Warm-up phenomenon | Present | Absent | | Autonomic symptoms | Common | Absent | | Reflexes | Diminished/absent | Normal | | Associated malignancy | SCLC (50–60%) | Thymoma (10–15%) | | Antibody target | P/Q-type VGCC | Nicotinic AChR | | RNS pattern | Decremental → incremental | Decremental | ### Management 1. **Malignancy screening:** Urgent CT chest if SCLC not yet diagnosed 2. **Symptomatic treatment:** 3,4-Diaminopyridine (3,4-DAP) — increases acetylcholine release 3. **Immunosuppression:** Corticosteroids, azathioprine, IVIG 4. **Treatment of underlying cancer:** Often leads to syndrome improvement **Clinical Pearl:** The "warm-up" phenomenon (transient improvement with muscle use) is a key distinguishing feature from myasthenia gravis and is highly suggestive of LEMS. 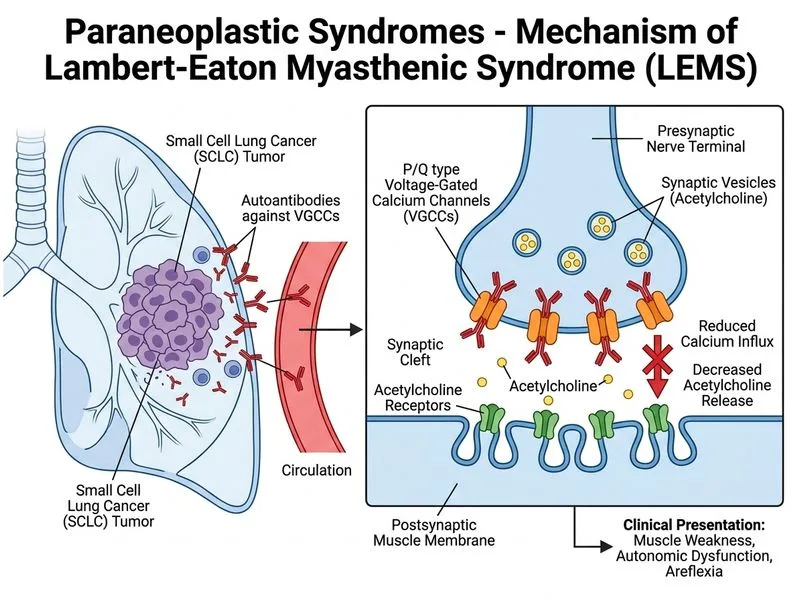
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.