## Diagnosis & Clinical Presentation **Key Point:** This patient meets diagnostic criteria for acute pelvic inflammatory disease (PID): pelvic pain + pelvic tenderness (cervical motion tenderness, adnexal tenderness) + evidence of inflammation (fever, elevated WBC, imaging findings). ## Management Strategy for Acute PID ### Severity Assessment This patient has **severe PID** warranting hospitalization because of: - Fever ≥38.5°C - Elevated WBC with left shift - Imaging evidence of salpingitis and free pelvic fluid - Risk of progression to tubo-ovarian abscess or sepsis ### Antibiotic Regimen **High-Yield:** The CDC-recommended inpatient regimen for PID is: | Component | Drug | Dose | Route | |-----------|------|------|-------| | **Cephalosporin** | Ceftriaxone | 1 g IV/IM q24h | IV/IM | | **Tetracycline** | Doxycycline | 100 mg IV/PO q12h | IV or PO | | **Anaerobic coverage** | Metronidazole | 500 mg IV q8h | IV | **Clinical Pearl:** The triple-agent regimen covers the polymicrobial nature of PID: - *Neisseria gonorrhoeae* (ceftriaxone) - *Chlamydia trachomatis* (doxycycline) - Anaerobes including *Bacteroides* and *Peptostreptococcus* (metronidazole) ### Duration & Follow-up - Continue IV therapy until clinical improvement (48–72 hours) - Then switch to oral doxycycline to complete 14 days total - Recheck vital signs and WBC at 48–72 hours **Mnemonic:** **PID-TRIPLE** = **P**elvic **I**nflammatory **D**isease → **T**riplet **R**egimen **I**V **P**lus **L**ater **E**xtended oral ## Why Hospitalization? 1. Fever and systemic toxicity 2. Imaging evidence of advanced disease 3. Risk of complications (abscess, sepsis) 4. Need for close monitoring and IV antibiotics [cite:Park 26e Ch 18] 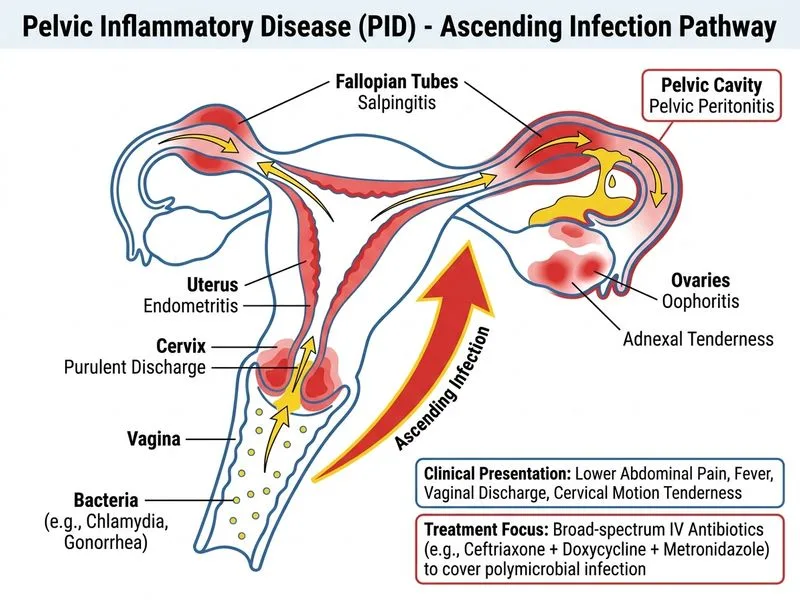
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.