## Diagnosis: Pelvic Inflammatory Disease with Tubo-Ovarian Abscess (TOA) — IUD-Associated ### Clinical Features of Severe PID with TOA | Feature | Finding | Significance | |---------|---------|---------------| | **Fever** | 39.2°C | Systemic infection | | **Toxicity** | Appears toxic | Indicates severe sepsis | | **Imaging** | 4 cm TOA with internal echoes | Abscess formation (>3 cm) | | **WBC** | 14,500 with left shift | Acute bacterial infection | | **IUD status** | In situ | Foreign body perpetuates infection | **Key Point:** A tubo-ovarian complex >3 cm with internal echoes on ultrasound is diagnostic of tubo-ovarian abscess (TOA) [cite:Park 26e Ch 21] ### Management Algorithm for IUD-Associated PID with TOA ```mermaid flowchart TD A[Severe PID + TOA + IUD]:::outcome --> B[Remove IUD immediately]:::urgent B --> C[Start IV broad-spectrum antibiotics]:::action C --> D[Ceftriaxone + Doxycycline + Metronidazole]:::action D --> E{Clinical improvement in 48-72 hours?}:::decision E -->|Yes| F[Continue IV antibiotics × 14 days total]:::action E -->|No| G[Diagnostic laparoscopy ± drainage]:::action G --> H{Abscess drained?}:::decision H -->|Yes| I[Continue IV antibiotics]:::action H -->|No| J[Consider open drainage/hysterectomy]:::urgent F --> K[Discharge on oral antibiotics to complete 14 days]:::action ``` ### Rationale for Correct Answer **High-Yield:** IUD removal is mandatory in PID because: 1. The IUD acts as a **foreign body** that perpetuates infection and abscess formation 2. Continuation of the IUD significantly increases risk of treatment failure and sepsis 3. Removal improves antibiotic penetration and reduces abscess recurrence [cite:Harrison 21e Ch 137] **Immediate antibiotic regimen for severe PID with TOA:** - **Ceftriaxone 1–2 g IV Q12H** (covers gram-negative organisms and *N. gonorrhoeae*) - **Doxycycline 100 mg IV/PO BD** (covers *Chlamydia* and gram-positive cocci) - **Metronidazole 500 mg IV TDS** (covers anaerobes, which are common in IUD-associated infection) **Clinical Pearl:** Diagnostic laparoscopy is reserved for patients who do NOT improve clinically within 48–72 hours of antibiotics. It allows visualization of the abscess, confirmation of diagnosis, and drainage if needed. Emergency laparotomy is only indicated if the abscess ruptures or the patient deteriorates acutely. ### Why 48–72 Hour Observation Before Laparoscopy? - ~50% of TOAs respond to antibiotics alone without drainage - Laparoscopy carries morbidity; reserve for treatment failures - If fever persists, imaging worsens, or peritonitis develops → proceed to laparoscopy 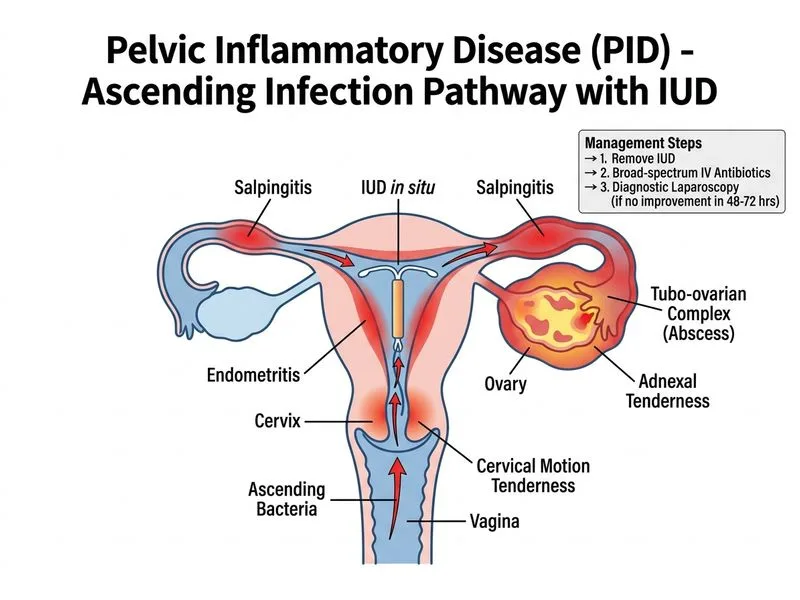
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.