This patient has had a partial response to initial salbutamol nebulization — peak flow improved from 180 to 280 L/min, but she remains dyspneic, tachypneic (RR 26/min), and hypoxic (SpO₂ 88%). This is an acute, life-threatening situation requiring immediate concurrent interventions.
These two interventions (repeat SABA + supplemental O₂) are the most immediate, direct, and life-saving steps and should occur before or simultaneously with systemic corticosteroids.
Systemic corticosteroids (Option D) are absolutely indicated in this scenario and should be initiated early — but their onset of action is 4–6 hours (genomic mechanism). They do not address the immediate hypoxemia or bronchospasm in the next few minutes. In standard acute asthma protocols (GINA 2023, BTS/SIGN), repeat SABA + oxygen is the first action, with corticosteroids added as a concurrent but slightly downstream step.
GINA 2023 Acute Asthma Protocol: Step 1 — Supplemental O₂ + repeated SABA (salbutamol) every 20 minutes. Step 2 — Add systemic corticosteroids early. Step 3 — Add ipratropium bromide. Step 4 — Consider IV magnesium sulfate for severe cases. The sequence matters: oxygen and repeat SABA are the first actions in a patient with SpO₂ 88%.
Reference: GINA Global Strategy for Asthma Management 2023; BTS/SIGN British Guideline on the Management of Asthma 2022; KD Tripathi Essentials of Medical Pharmacology 8th ed.
Loading illustration…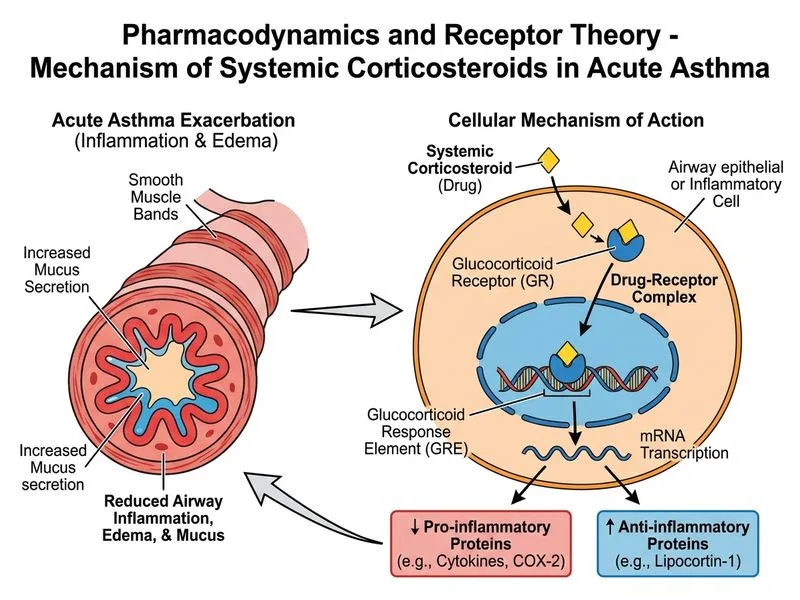
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →