## Radial Nerve Injury During Axillary Dissection **Nerve Anatomy and Course:** - **Origin:** Terminal branch of the posterior cord (C5–C6–C7–C8) - **Course in axilla:** Runs posterior to the axillary artery, then travels posteriorly to enter the spiral groove of the humerus - **Motor innervation:** - Triceps (elbow extension) - Extensor carpi radialis longus and brevis (wrist extension) - Extensor carpi ulnaris (wrist extension) - Extensor digitorum (finger extension) - Extensor pollicis longus (thumb extension) - Abductor pollicis longus **Clinical Presentation Analysis:** - **Wrist drop** → Loss of wrist extensors (extensor carpi radialis/ulnaris) - **Loss of thumb extension** → Extensor pollicis longus paralyzed - **Preserved elbow flexion** → Musculocutaneous nerve intact - **Preserved shoulder abduction** → Axillary nerve intact **Anatomical Vulnerability:** The radial nerve is vulnerable during axillary dissection because: 1. It runs **posteriorly in the axilla** along the axillary artery 2. It is **stretched during traction** of the axillary contents during lymph node dissection 3. The nerve can be **compressed or lacerated** by retractors or direct manipulation 4. Its posterior location makes it less obvious during the dissection compared to anterior structures **High-Yield Fact:** Radial nerve injury during axillary dissection is one of the most common nerve injuries in breast surgery, occurring in 0.5–2% of cases. **Clinical Pearl:** Wrist drop + thumb extension loss = radial nerve injury until proven otherwise. 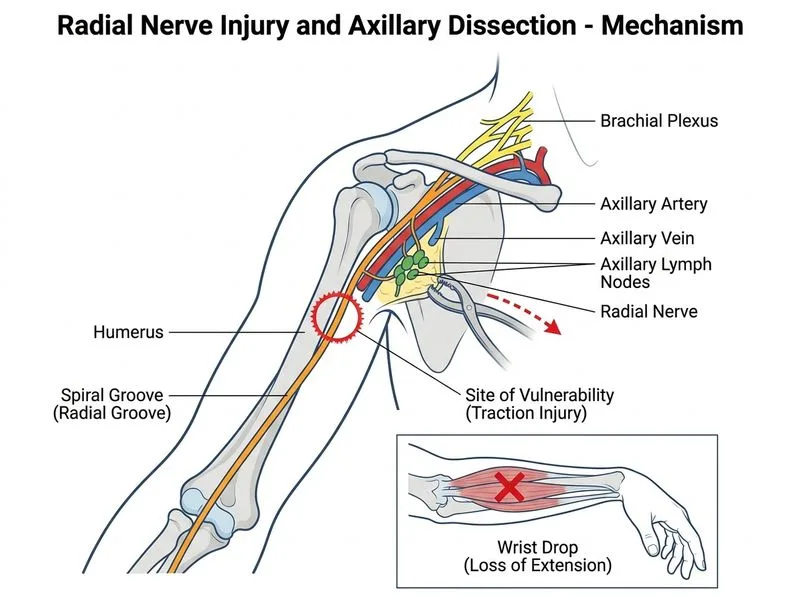
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.