## Clinical Diagnosis This patient presents with **acute hemorrhagic pancreatitis with hypovolemic shock**: **Key Point:** The clinical triad is: 1. **Acute severe pancreatitis** — epigastric pain, elevated amylase (1240 U/L), vomiting 2. **Hypovolemic shock** — severe hypotension (76/48), tachycardia (132), cold/clammy skin, poor response to initial fluid bolus 3. **Peritoneal hemorrhage** — free fluid on ultrasound, rigid abdomen, absent bowel sounds ## Shock Classification: Why Hypovolemic? | Shock Type | Mechanism | BP Response to Fluids | Lactate | Skin | Next Step | |---|---|---|---|---|---| | **Hypovolemic** | Blood/fluid loss | Poor after 2 L | Elevated | Cold, clammy | **Surgery** | | Cardiogenic | Pump failure | Pulmonary edema | Elevated | Cold | Inotropes, imaging | | Septic | Infection + vasodilation | Good initially | Elevated | Warm initially | Antibiotics, vasopressors | | Distributive | Vasodilation (anaphylaxis, etc.) | Good with fluids | Elevated | Warm, flushed | Epinephrine (anaphylaxis) | **High-Yield:** Hemorrhagic pancreatitis causes **retroperitoneal bleeding** that pools fluid and blood in the peritoneum, creating a "third space" loss. Crystalloid alone cannot restore intravascular volume fast enough; **surgical hemostasis is mandatory**. ## Why Immediate Surgery? 1. **Persistent shock despite 2 L crystalloid** → indicates ongoing hemorrhage, not simple dehydration 2. **Free peritoneal fluid + rigid abdomen** → suggests active bleeding or perforation requiring operative intervention 3. **Severe acute pancreatitis with hemodynamic collapse** → high mortality if not surgically managed (mortality ~30–50% in hemorrhagic pancreatitis with shock) **Clinical Pearl:** In hemorrhagic pancreatitis, the retroperitoneum can sequester 6–10 liters of blood. Fluid resuscitation alone is temporizing; definitive control requires surgery (angiographic embolization or open hemostasis). ## Why Not the Other Options? - **Cardiogenic shock (option B):** No cardiac history, no chest pain, no ECG changes suggested. Cold extremities and poor fluid response fit hypovolemic, not cardiogenic, shock. Dobutamine would worsen hypotension in a hypovolemic patient. - **Septic shock (option C):** No fever, no infection source (pancreatitis is not inherently infectious at presentation). Amylase elevation is from pancreatic necrosis, not infection. Antibiotics alone will not stop bleeding. - **Distributive shock (option D):** Warm, flushed skin is typical of distributive shock; this patient is cold and clammy (vasoconstricted), indicating hypovolemia. Continued fluid administration without surgery will delay critical intervention. 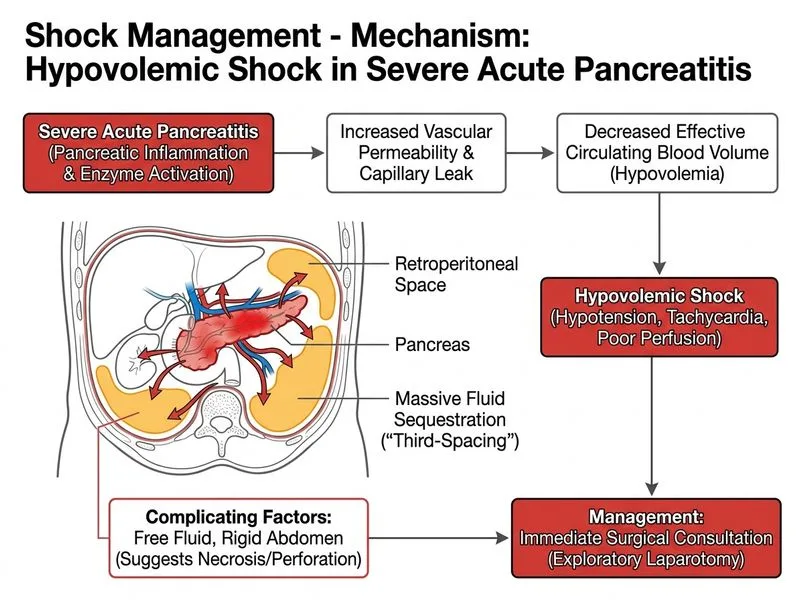
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.