## Clinical Diagnosis This patient has **septic shock** secondary to community-acquired pneumonia (CAP) with evidence of organ dysfunction (altered mental status, hypotension, tachycardia, metabolic acidosis with elevated lactate). ## Sepsis-3 Criteria Met **Key Point:** Septic shock = infection + hypotension requiring vasopressors + elevated lactate ≥2 mmol/L despite adequate fluid resuscitation. This patient meets all criteria: - Suspected infection (fever, respiratory symptoms, bilateral infiltrates) - Hypotension: 88/54 mmHg - Lactate: 4.2 mmol/L (>2) - Altered mental status (confusion) ## Surviving Sepsis Campaign (SSC) 2021 Bundle — 1-Hour Targets | Intervention | Target | Rationale | |---|---|---| | Fluid bolus | 30 mL/kg crystalloid | Restore intravascular volume; improves microcirculation | | Blood cultures | Before antibiotics | Maximize culture yield | | Broad-spectrum antibiotics | Within 1 hour | Empiric coverage for gram-positive, gram-negative, atypicals | | Lactate measurement | Baseline + reassess | Marker of tissue hypoperfusion; guides resuscitation | | Vasopressors | If SBP <65 mmHg after fluids | Noradrenaline is first-line | **High-Yield:** The 30 mL/kg bolus is given **upfront**, not after observation. Early aggressive resuscitation reduces mortality in septic shock. ## Why Fluids First, Then Vasopressors 1. **Hypovolemia is the primary problem** in septic shock (capillary leak, vasodilation). 2. Fluid resuscitation restores preload and improves cardiac output. 3. Vasopressors are **adjunctive** — used only if hypotension persists after adequate fluid loading. 4. Premature vasopressor use without fluid resuscitation worsens tissue perfusion and organ failure. **Clinical Pearl:** Warm extremities + hypotension + high lactate = distributive shock requiring fluid resuscitation as the cornerstone of initial therapy. ## Bilateral Infiltrates Do Not Contraindicate Fluid Bolus **Warning:** The presence of pulmonary infiltrates does NOT mean you should withhold fluids. The infiltrates may reflect: - Pneumonia (primary infection) - ARDS (secondary to sepsis) - Pulmonary edema (but this is a *late* complication if fluids are excessive and prolonged) The **30 mL/kg bolus over 1 hour** is safe and guideline-mandated. Monitor for response (BP, lactate clearance, urine output). If pulmonary edema develops, switch to vasopressors and consider diuretics, not fluid restriction from the start. ## Treatment Algorithm ```mermaid flowchart TD A[Septic shock suspected]:::outcome --> B[Obtain blood cultures]:::action B --> C[Start broad-spectrum antibiotics]:::action C --> D[30 mL/kg crystalloid bolus]:::action D --> E{Response to fluids?}:::decision E -->|SBP ≥65, lactate ↓| F[Continue fluids, reassess]:::action E -->|SBP <65 or persistent hypotension| G[Start noradrenaline]:::action G --> H[Target MAP ≥65 mmHg]:::action H --> I[Reassess lactate at 3 hours]:::action ``` [cite:Harrison 21e Ch 297] 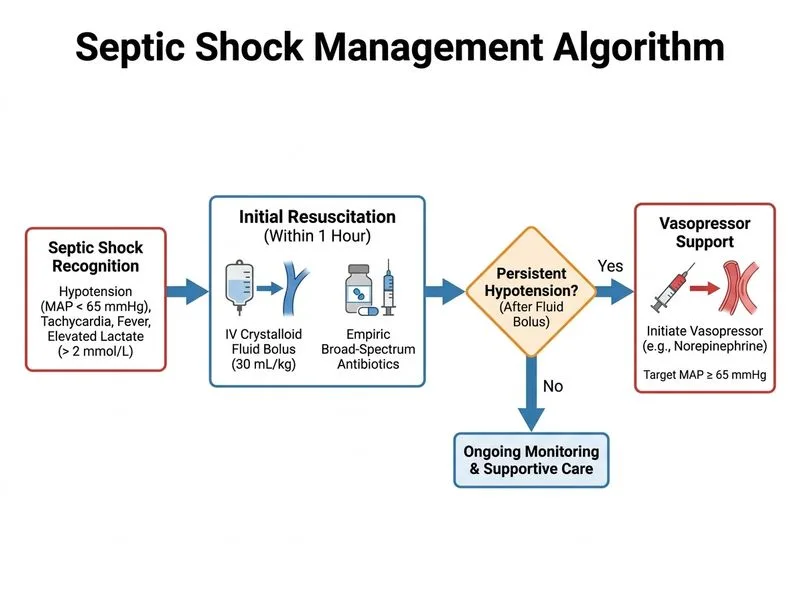
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.