## Diagnosis: Cardiogenic Shock Secondary to Acute MI with Mechanical Complication **Key Point:** This patient has **cardiogenic shock** — hypotension due to **acute reduction in cardiac output** from myocardial infarction. The new pansystolic murmur suggests acute mitral regurgitation from papillary muscle rupture or dysfunction, further compromising forward flow. ### Pathophysiology of Cardiogenic Shock ```mermaid flowchart TD A[Acute MI - Loss of >40% LV mass]:::outcome --> B[Reduced LV contractility]:::action B --> C[Decreased Stroke Volume]:::outcome C --> D[Decreased Cardiac Output<br/>CO = SV × HR]:::action D --> E[Systemic Hypoperfusion]:::urgent A --> F[Papillary Muscle Rupture/<br/>Dysfunction]:::urgent F --> G[Acute Mitral Regurgitation]:::outcome G --> H[Reduced Forward Flow &<br/>Increased LA Pressure]:::action H --> I[Pulmonary Edema &<br/>Respiratory Failure]:::urgent E --> J[Tissue Hypoxia &<br/>Anaerobic Metabolism]:::outcome J --> K[Metabolic Acidosis &<br/>Lactate Elevation]:::outcome ``` ### Clinical Features Distinguishing Cardiogenic Shock | Feature | Cardiogenic Shock | Septic Shock | Hypovolemic Shock | |---------|-------------------|--------------|-------------------| | **Skin** | Cool, pale, clammy | Warm, flushed | Cool, clammy | | **JVP** | Elevated (8–12 cm H₂O) | Normal or low | Low (<2 cm H₂O) | | **Lung sounds** | Crackles (pulmonary edema) | Clear or crackles | Clear | | **Cardiac output** | Reduced | High (early) or low (late) | Reduced | | **SVR** | Elevated (compensatory) | Low (vasodilation) | Elevated | | **Cause** | Pump failure | Distributive (infection) | Volume loss | **High-Yield:** The **triad of cardiogenic shock** = Hypotension + Elevated JVP + Pulmonary edema. This patient has all three. ### Why This Is Cardiogenic, Not Distributive Shock **Clinical Pearl:** The **elevated JVP (8 cm H₂O) + pulmonary crackles + pale, clammy skin** indicate **backward failure** (pulmonary congestion) and **reduced forward flow** (hypoperfusion). This is the hallmark of cardiogenic shock. - In **septic shock**, JVP is normal or low, skin is warm (vasodilation), and crackles reflect ARDS, not cardiogenic pulmonary edema. - In **hypovolemic shock**, JVP is low (<2 cm H₂O), and there is no pulmonary edema. ### Mechanical Complication: Acute Mitral Regurgitation The **new pansystolic (holosystolic) murmur** at the apex indicates acute mitral regurgitation from: 1. **Papillary muscle rupture** (posteromedial > anterolateral) 2. **Papillary muscle dysfunction** from ischemia 3. **Annular dilation** from LV remodeling This worsens cardiogenic shock by: - Reducing forward stroke volume - Increasing left atrial pressure → pulmonary edema - Increasing myocardial oxygen demand **Mnemonic: SHOCK classification for acute MI complications** — **S**eptal rupture, **H**eart failure/cardiogenic shock, **O**utflow obstruction, **C**ontainment rupture, **K**inetic abnormality (papillary muscle rupture). ### Laboratory Findings - **pH 7.32, HCO₃⁻ 18** → Metabolic acidosis from tissue hypoperfusion - **PaCO₂ 38** → Respiratory compensation is inadequate (should be <30 in pure metabolic acidosis) → suggests concurrent respiratory failure from pulmonary edema [cite:Robbins 10e Ch 4; Harrison 21e Ch 297] 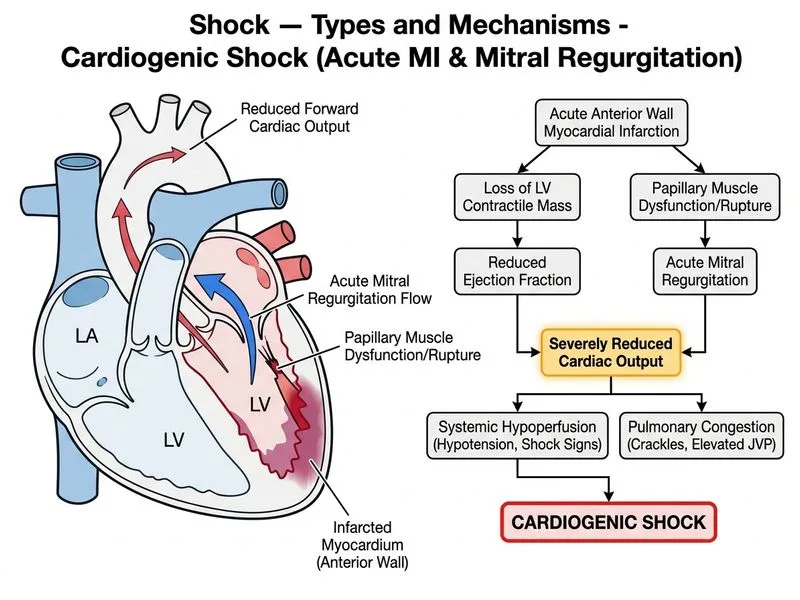
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.