## Clinical Presentation Analysis **Key Point:** This patient has **anterior wall STEMI** (ST elevation V1–V4) complicated by **acute cardiogenic shock** (BP 95/60, HR 118, RR 24, SpO₂ 88%) and **acute pulmonary edema**, raising strong suspicion for a **mechanical complication** — specifically **acute mitral regurgitation (MR) from papillary muscle rupture**. ## Why Papillary Muscle Rupture? **High-Yield:** Papillary muscle rupture is the most feared mechanical complication of STEMI causing acute, severe MR. The **posteromedial papillary muscle** is most commonly affected (single blood supply from RCA or LCx), but in large anterior STEMIs involving the LAD, the **anterolateral papillary muscle** can also be affected. Even in anterior STEMI, papillary muscle ischemia/necrosis can occur due to the extensive territory of infarction. **Clinical Pearl:** The classic triad pointing to papillary muscle rupture: 1. **Acute STEMI** (anterior or inferior) 2. **Flash pulmonary edema** (sudden volume overload from severe MR) 3. **Cardiogenic shock** (loss of forward cardiac output) 4. **New holosystolic murmur** (acute MR — though not always audible in low-output states) **Temporal Note:** While papillary muscle rupture classically occurs **3–7 days post-MI** (peak necrosis), it can occur acutely (within hours) in the setting of **massive transmural infarction** with complete papillary muscle necrosis, as implied by this patient's markedly elevated troponin (2.8 ng/mL) and hemodynamic collapse at 90 minutes. This acute presentation, though less common, is well-recognized in the literature (Harrison's Principles of Internal Medicine, 21e, Ch. 297). ## Differential Diagnosis of Mechanical Complications | Complication | Timing | Presentation | Key Finding | Murmur | |---|---|---|---|---| | **Papillary Muscle Rupture** | 3–7 days (acute: massive MI) | Flash pulmonary edema, shock | Flail mitral leaflet on echo; V-wave on PAWP | Holosystolic at apex | | **VSD Rupture** | 3–5 days | Biventricular failure, step-up in O₂ sat | Left-to-right shunt on echo | Pansystolic at left sternal border | | **Free Wall Rupture** | 3–6 days | Sudden collapse, tamponade physiology | Pericardial effusion, electrical alternans | None | | **Dressler Syndrome** | 2–8 weeks post-MI | Fever, pleurisy, pericarditis | Pericardial friction rub | None | ## Why Not the Other Options? - **A (VSD):** VSD from septal rupture causes a left-to-right shunt with a harsh pansystolic murmur at the left sternal border and oxygen step-up in the RV — not predominantly pulmonary edema and shock without mention of RV failure. - **B (Dressler syndrome):** Occurs 2–8 weeks post-MI; presents with fever, pleurisy, and pericarditis — not acute cardiogenic shock at 90 minutes. - **C (Free wall rupture):** Causes tamponade physiology (Beck's triad: hypotension, JVD, muffled heart sounds) and electrical alternans — not bilateral pulmonary edema. ## Diagnostic Confirmation - **Echocardiography (Gold Standard):** Flail mitral leaflet, severe MR jet, ruptured papillary muscle head - **Pulmonary artery catheter:** Prominent V-wave on pulmonary artery wedge pressure (PAWP) - **Chest X-ray:** Bilateral pulmonary edema (as seen here) **Warning:** Acute papillary muscle rupture is a **surgical emergency**. Mortality without surgery approaches 80–100%; with urgent surgical repair or replacement, mortality is 20–40% (Harrison 21e, Ch. 297). [cite:Harrison 21e Ch 297] 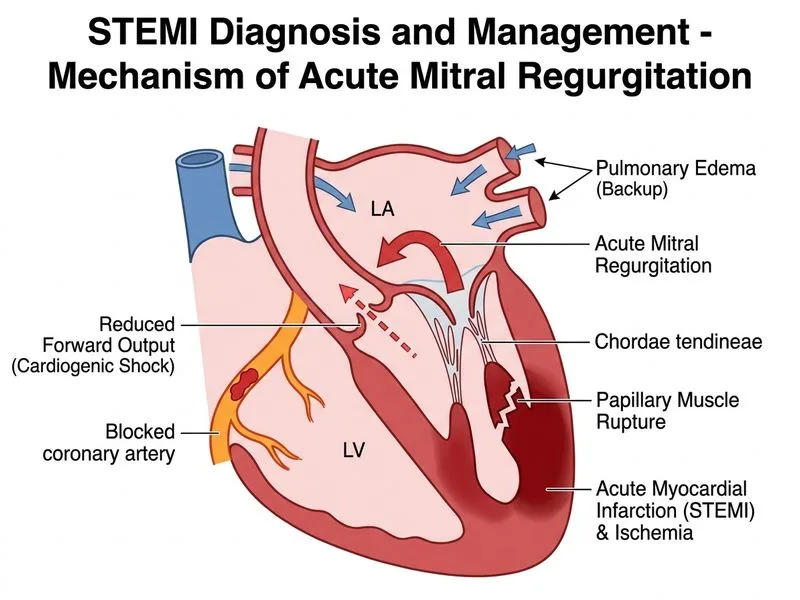
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.