STEMI Diagnosis and Management MCQ — NEET PG Practice Question | NEETPGAI
STEMI Diagnosis and Management
medium
stethoscope Medicine
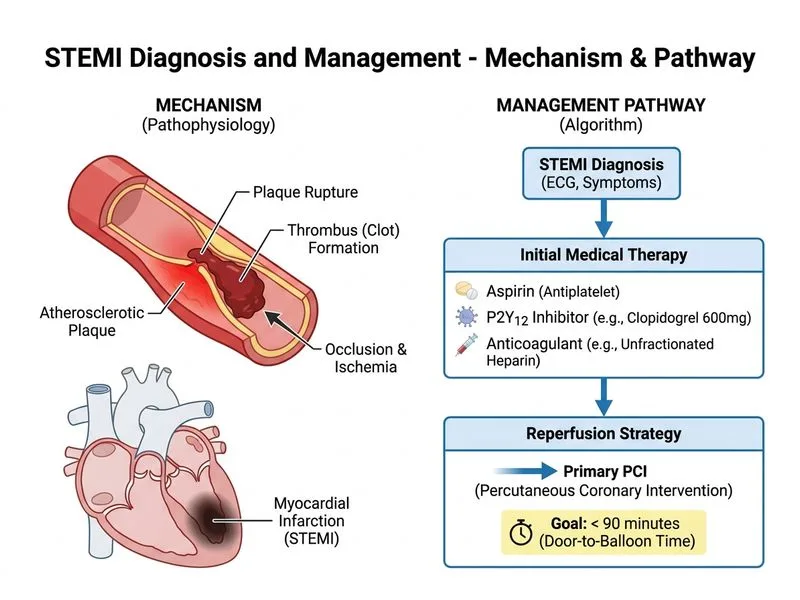
A 58-year-old man with a 10-year history of hypertension and type 2 diabetes presents to the emergency department with acute-onset crushing substernal chest pain radiating to the left arm, associated with diaphoresis and nausea for the past 2 hours. On examination, blood pressure is 145/92 mmHg, heart rate 102/min, and respiratory rate 20/min. A 12-lead ECG shows ST-segment elevation of 3 mm in leads II, III, and aVF, with reciprocal ST depression in leads I and aVL. Troponin I is 0.8 ng/mL (normal <0.04). The patient is on aspirin 75 mg daily at home. What is the most appropriate immediate management?
A. Administer loading dose of clopidogrel 600 mg, unfractionated heparin bolus, and arrange primary percutaneous coronary intervention within 90 minutes
B. Administer intravenous nitroglycerin, oral beta-blocker, and arrange coronary angiography within 24 hours
C. Administer aspirin 300 mg loading dose, enoxaparin, and observe with serial ECGs and troponins
D. Administer loading dose of ticagrelor 180 mg, morphine, and proceed to thrombolysis with streptokinase
Explanation
Diagnosis: Inferior Wall STEMI
Key Point
This patient presents with acute ST-elevation myocardial infarction (STEMI) of the inferior wall, evidenced by ST elevation in the inferior leads (II, III, aVF) with reciprocal changes and elevated troponin in the appropriate clinical context.
Immediate Management Strategy
High-YieldNEET PG
The 2017 ESC and 2015 ACC/AHA guidelines mandate primary percutaneous coronary intervention (PCI) as the gold standard reperfusion strategy for STEMI when performed by an experienced team within 120 minutes (ideally 90 minutes) of first medical contact.
Step-by-Step Approach:
1.
Dual antiplatelet therapy (DAPT):
Aspirin 300–500 mg loading dose (already on 75 mg maintenance)
P2Y₁₂ inhibitor loading: Clopidogrel 600 mg OR ticagrelor 180 mg OR prasugrel 60 mg
Clopidogrel is preferred in this case because ticagrelor requires IV access and has more bleeding risk in elderly; prasugrel contraindicated if age >75 or weight <60 kg
2.
Anticoagulation:
Unfractionated heparin (UFH) bolus: 70–100 U/kg IV (preferred during PCI for easier reversal)
Alternative: Enoxaparin 0.5 mg/kg IV if PCI delayed
3.
Reperfusion:
Primary PCI within 90 minutes is superior to thrombolysis in reducing mortality, reinfarction, and stroke
No contraindication to PCI in this patient
4.
Adjunctive therapy:
IV nitroglycerin (if SBP >90 mmHg and no RV involvement)
Beta-blocker (metoprolol 25–50 mg) to reduce heart rate and myocardial oxygen demand
Morphine for analgesia and anxiolysis
Clinical Pearl
Inferior STEMI may involve the right ventricle (RV infarction) — assess for elevated JVP or hypotension with bradycardia. RV infarction is preload-dependent; avoid nitrates and diuretics; consider IV fluids if RV involvement suspected.
Why This Option is Correct
Option 0 combines DAPT (clopidogrel 600 mg loading) + UFH + primary PCI, which aligns with guideline-recommended reperfusion strategy and achieves the fastest door-to-balloon time for STEMI.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.