STEMI Diagnosis and Management MCQ — NEET PG Practice Question | NEETPGAI
STEMI Diagnosis and Management
hard
stethoscope Medicine
A 52-year-old woman with no prior cardiac history presents to the emergency department with acute-onset severe anterior chest pain and diaphoresis for 90 minutes. She is a current smoker and takes oral contraceptives. On examination, blood pressure is 110/70 mmHg, heart rate 88/min. A 12-lead ECG obtained at 15 minutes shows ST-segment elevation of 2.5 mm in leads V1–V4 with reciprocal ST depression in leads II, III, and aVF. High-sensitivity troponin is 0.05 ng/mL (upper limit of normal 0.04). The nearest PCI-capable hospital is 180 km away with an estimated transport time of 3 hours. What is the most appropriate reperfusion strategy?
A. Administer aspirin and heparin, and observe with serial troponins while arranging transfer for angiography
B. Administer aspirin, clopidogrel, and initiate fibrinolytic therapy with alteplase immediately, with plan for rescue PCI if reperfusion fails
C. Administer aspirin, clopidogrel, and nitroglycerin, and defer reperfusion pending repeat ECG in 30 minutes
D. Administer aspirin, clopidogrel, and arrange immediate transfer for primary PCI, accepting the 3-hour door-to-balloon time
Explanation
Diagnosis: Anterior Wall STEMI
Key Point
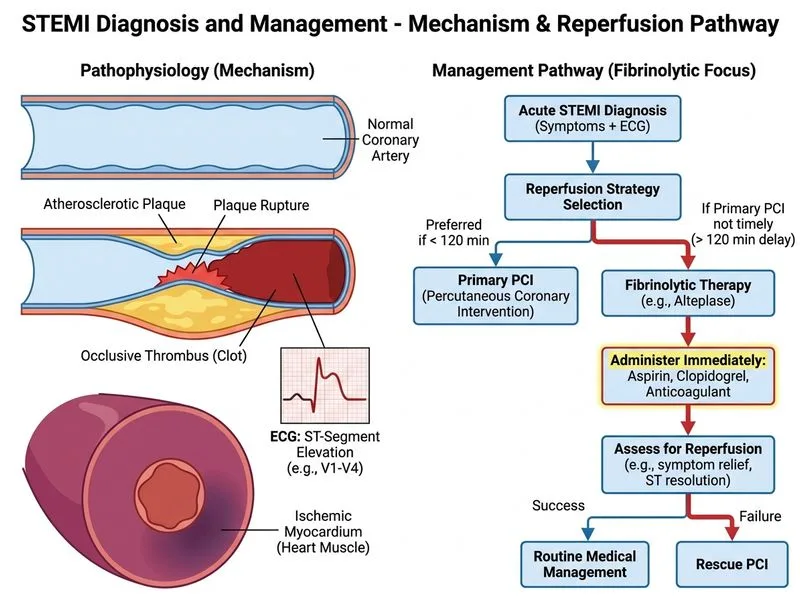
This patient has acute anterior STEMI (ST elevation in V1–V4, reciprocal changes, elevated troponin) with a door-to-PCI time of 180 minutes, which exceeds the recommended 120-minute window. In this scenario, fibrinolytic therapy is the preferred reperfusion strategy.
Reperfusion Strategy Selection
Guideline-Based Decision Tree:
Loading diagram...
High-YieldNEET PG
The 2017 ESC and 2015 ACC/AHA guidelines state:
Primary PCI is preferred if door-to-balloon time ≤120 minutes (ideally ≤90 min)
Fibrinolytic therapy is preferred if PCI cannot be performed within 120 minutes
Fibrinolysis should be initiated within 30 minutes of first medical contact ("door-to-needle" ≤30 min)
This Patient's Scenario:
Door-to-PCI time = 180 minutes (exceeds 120-minute guideline threshold)
Therefore: Fibrinolytic therapy is the appropriate choice
Fibrinolytic Agent Selection
Table
Agent
Fibrin-Specificity
Reperfusion Rate
Bleeding Risk
Dosing
Alteplase (tPA)
High
70–80%
Moderate
15 mg IV bolus, then 0.75 mg/kg over 30 min, then 0.5 mg/kg over 60 min
Streptokinase
Low
60–70%
Lower
1.5 MU IV over 60 min
Reteplase
High
75–80%
Moderate
10 U IV bolus × 2 (30 min apart)
Tenecteplase
High
80–85%
Moderate
Weight-based single bolus
Clinical Pearl
Alteplase is preferred in anterior STEMI due to superior reperfusion rates and lower reinfarction risk compared to streptokinase, despite slightly higher bleeding risk.
Anticoagulation: UFH bolus 60 U/kg (max 4000 U) followed by infusion, OR enoxaparin 0.3 mg/kg IV
3.
Beta-blocker: Metoprolol 25–50 mg (if no contraindications)
4.
Rescue PCI: If ECG shows <50% ST-segment resolution at 60–90 minutes post-fibrinolysis, proceed to rescue PCI
Warning
Do NOT delay fibrinolysis waiting for transfer or repeat ECG. Time is myocardium — every 30-minute delay increases 1-year mortality by ~7.5%.
Why This Option is Correct
Option 1 combines immediate fibrinolytic therapy (alteplase) + DAPT, which is guideline-concordant when PCI cannot be performed within 120 minutes. The plan for rescue PCI if reperfusion fails ensures safety and optimal outcomes.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.