A 28-year-old woman with recurrent episodes of muscle pain and weakness is found to have elevated serum lactate and pyruvate levels. Genetic testing reveals a mutation in the E1α subunit of pyruvate dehydrogenase complex. Which metabolic finding best distinguishes her condition from a deficiency of succinate dehydrogenase?
A. Elevated lactate-to-pyruvate ratio with normal citrate levels
B. Reduced α-ketoglutarate levels with normal pyruvate metabolism
C. Elevated pyruvate and lactate with impaired entry into TCA cycle at the acetyl-CoA formation step
D. Elevated acetyl-CoA with decreased NADH production
Explanation
Distinguishing PDH Deficiency from Succinate Dehydrogenase (SDH) Deficiency
Pyruvate Dehydrogenase Complex (PDH) Deficiency
Key Point
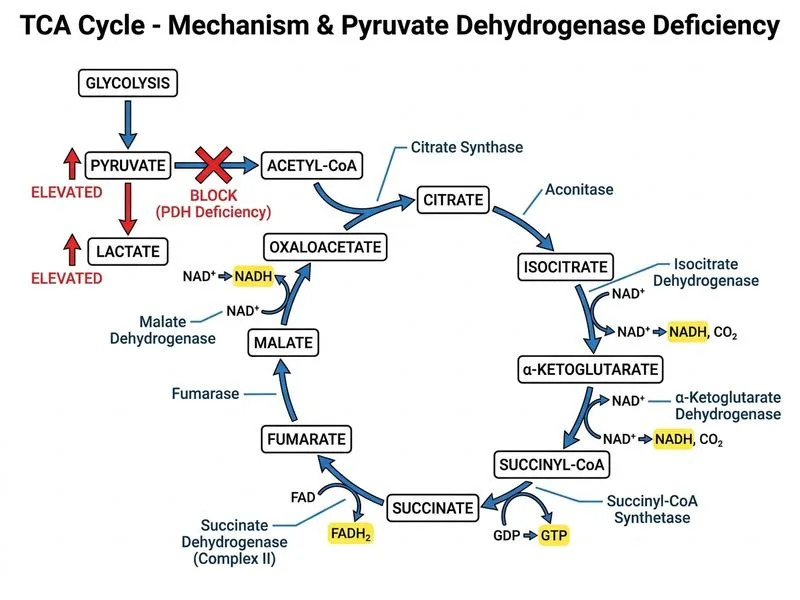
PDH deficiency blocks the entry point of the TCA cycle. Pyruvate cannot be converted to acetyl-CoA, causing:
Accumulation of pyruvate upstream
Shunting of pyruvate to lactate via lactate dehydrogenase (LDH)
Elevated pyruvate AND lactate (lactic acidosis)
Reduced acetyl-CoA availability
Impaired energy production and NADH generation
High-YieldNEET PG
The hallmark is elevated pyruvate and lactate with blocked TCA cycle entry — this is the classic presentation of PDH deficiency.
Succinate Dehydrogenase (SDH) Deficiency
Key Point
SDH deficiency blocks an intermediate step within the TCA cycle (succinate → fumarate). The metabolic consequences are:
Accumulation of succinate and upstream intermediates (α-ketoglutarate, isocitrate, citrate)
Normal pyruvate metabolism (PDH still functions)
Pyruvate and lactate remain normal or only mildly elevated
Impaired FADH2 generation (SDH is Complex II of the electron transport chain)
Progressive accumulation of TCA intermediates
Comparative Metabolic Profiles
Table
Metabolic Parameter
PDH Deficiency
SDH Deficiency
Pyruvate
↑↑ Elevated
Normal or slightly ↑
Lactate
↑↑ Elevated (lactic acidosis)
Normal or slightly ↑
Citrate
↓ Low (blocked entry)
↑ Elevated (blocked exit)
α-Ketoglutarate
↓ Low (blocked entry)
↑ Elevated (blocked exit)
Succinate
Normal
↑↑ Markedly elevated
NADH
↓ Reduced
↓ Reduced (but less than PDH)
FADH2
Normal
↓ Severely reduced
TCA Cycle Status
Blocked at entry
Blocked at intermediate step
Pathophysiology Flowchart
Loading diagram...
Clinical Pearl
PDH deficiency presents with acute lactic acidosis during metabolic stress (infection, exercise), whereas SDH deficiency presents with progressive mitochondrial dysfunction and may cause paragangliomas or pheochromocytomas (familial SDH mutations are associated with SDHB/C/D tumors).
Mnemonic
PDH = Pyruvate Pileup — pyruvate and lactate accumulate because the entry gate to the TCA cycle is blocked. SDH = Succinate Stuck — succinate and upstream intermediates accumulate because an intermediate gate is blocked.
Why This Distinguishes the Conditions
The elevated pyruvate AND lactate with impaired TCA cycle entry at the acetyl-CoA formation step is pathognomonic for PDH deficiency. In SDH deficiency, pyruvate metabolism is normal, so pyruvate and lactate levels remain relatively normal — the blockade is downstream, not at the entry point.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.