## Diagnosis: Follicular Carcinoma ### Clinical Presentation The patient presents with a solitary thyroid nodule with normal TSH, which is a typical presentation for follicular thyroid neoplasm. The firm, mobile nodule with gradual enlargement over months is consistent with a slow-growing malignancy. ### Key Histopathologic Features **Key Point:** The diagnosis of follicular carcinoma is made on the basis of **capsular invasion** and/or **vascular invasion**, NOT on cytologic atypia alone. The FNAC report of "follicular neoplasm" reflects the cytologic limitation — FNAC cannot reliably distinguish benign follicular adenoma from follicular carcinoma because both show follicular architecture. The critical finding here is the **core needle biopsy demonstrating invasion through the thyroid capsule into surrounding adipose tissue**, which is the hallmark of malignancy in follicular lesions. ### Distinguishing Features: Follicular Adenoma vs. Carcinoma | Feature | Follicular Adenoma | Follicular Carcinoma | |---------|-------------------|----------------------| | **Capsular invasion** | Absent or incomplete | Present (complete) | | **Vascular invasion** | Absent | Present (diagnostic) | | **Mitotic activity** | Low | May be increased | | **Necrosis** | Rare | Can occur | | **Diagnosis method** | Histology (requires capsule assessment) | Histology (capsular/vascular invasion) | **High-Yield:** FNAC alone cannot diagnose follicular carcinoma — you MUST have histology showing invasion. ### Why This Is Not Other Carcinomas - **Papillary carcinoma**: Would show characteristic nuclear features ("Orphan Annie eye" nuclei, nuclear grooves, pseudoinclusions) on FNAC itself; capsular invasion is not the defining feature. - **Medullary carcinoma**: Would show C-cell origin with calcitonin positivity; presents differently (often familial, elevated calcitonin). **Clinical Pearl:** Follicular carcinoma has a better prognosis than papillary carcinoma when confined to the thyroid, but worse prognosis if distant metastases are present (especially bone and lung). ### Management Implication Once capsular invasion is confirmed histologically, total thyroidectomy followed by radioactive iodine ablation is indicated, unlike follicular adenoma which requires only lobectomy. 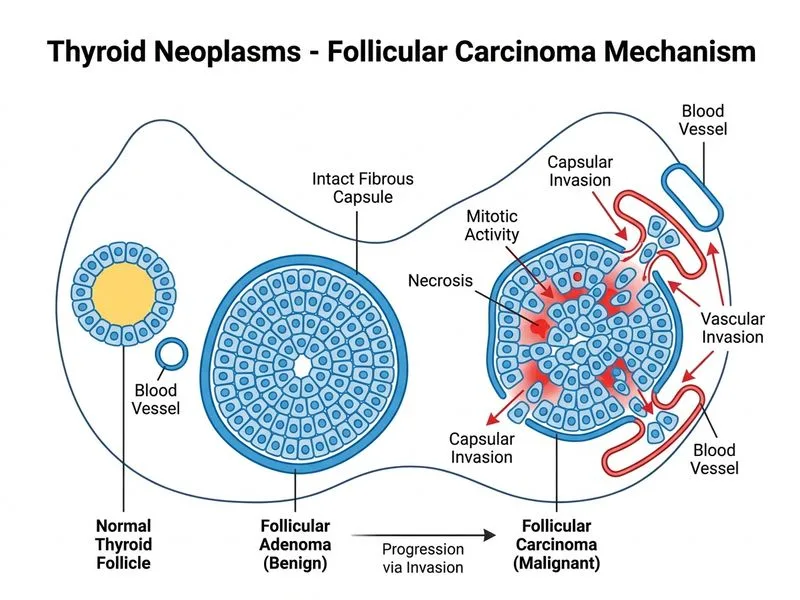
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.