Thyroid Neoplasms MCQ — NEET PG Practice Question | NEETPGAI
Thyroid Neoplasms
hard
microscope Pathology
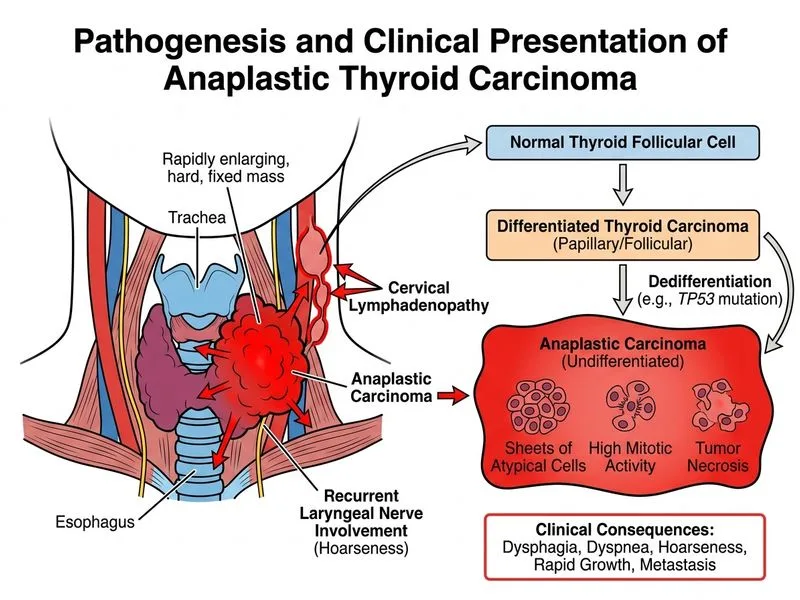
A 35-year-old woman from Delhi presents with a 6-month history of a rapidly enlarging thyroid mass associated with dysphagia and dyspnea. On examination, she has a hard, fixed thyroid mass with ipsilateral cervical lymphadenopathy. TSH is normal. Core needle biopsy shows sheets of atypical cells with high mitotic activity, tumor necrosis, and loss of follicular architecture. Immunohistochemistry is positive for p53 and negative for thyroglobulin. What is the most likely diagnosis?
A. Primary thyroid lymphoma
B. Papillary carcinoma with tall cell variant
C. Anaplastic carcinoma of thyroid
D. Medullary carcinoma of thyroid
Explanation
Diagnosis: Anaplastic Carcinoma of Thyroid
Clinical Presentation
The rapid growth, dysphagia, dyspnea, and fixed mass with cervical lymphadenopathy are hallmark features of anaplastic carcinoma. This is the most aggressive thyroid malignancy, with a median survival of 3–6 months if untreated.
High-YieldNEET PG
Anaplastic carcinoma accounts for only 1–2% of thyroid cancers but is responsible for up to 50% of thyroid cancer deaths due to its aggressive behavior.
Pathological Features
Table
Feature
Anaplastic Carcinoma
Differentiation
Undifferentiated (loss of follicular architecture)
Cell type
Spindle cells, giant cells, or pleomorphic cells
Mitotic activity
Very high (brisk)
Necrosis
Prominent tumor necrosis
Capsular invasion
Present (often with extrathyroidal extension)
Lymph node involvement
Common
Distant metastases
Frequent (lung, bone, brain)
Immunohistochemistry
Key Point
Anaplastic carcinoma is negative for thyroglobulin and thyroid peroxidase (TPO) because it has lost differentiation. The positive p53 indicates loss of p53 tumor suppressor function, a hallmark of anaplastic transformation.
Clinical Pearl
Anaplastic carcinoma often arises from pre-existing differentiated thyroid cancer (papillary or follicular) through a process of dedifferentiation. This explains why some patients have a prior history of thyroid cancer.
Diagnostic Criteria
1.
Undifferentiated histology: Loss of follicular pattern, sheets of atypical cells
2.
High mitotic rate: Brisk mitotic activity with abnormal mitoses
3.
Tumor necrosis: Extensive areas of necrosis
4.
Negative for thyroglobulin: Loss of thyroid differentiation markers
5.
Positive for p53, TP53 mutations: Indicates malignant transformation
TNM Staging
All anaplastic carcinomas are classified as Stage IV: