## Clinical Context The patient presents with classic features of pancreatic head cancer: painless jaundice, dilated intrahepatic bile ducts, and a hypoechoic pancreatic mass. This is an adenocarcinoma of the pancreas. ## Tumor Marker Selection for Pancreatic Cancer **Key Point:** CA 19-9 is the most clinically useful tumor marker for pancreatic adenocarcinoma. It is used for: - Diagnosis support (elevated in ~80% of pancreatic cancers) - Prognostic stratification (baseline level correlates with stage and survival) - Monitoring treatment response post-surgery or chemotherapy - Early detection of recurrence **High-Yield:** CA 19-9 is a Lewis blood group antigen-related carbohydrate antigen. Patients who are Lewis antigen-negative (~10% of population) will not produce CA 19-9 even with pancreatic cancer, so negative results do not exclude disease in these individuals. ## Comparison of Markers in Pancreatic Cancer | Marker | Sensitivity | Specificity | Clinical Use | |--------|-------------|-------------|---------------| | CA 19-9 | ~80% | ~90% | Primary marker; monitoring | | CEA | ~40% | ~80% | Non-specific; used in colorectal cancer | | AFP | <5% | High | Specific for hepatocellular carcinoma | | PSA | Not elevated | N/A | Specific for prostate cancer | **Clinical Pearl:** A rising CA 19-9 level during or after treatment (even before imaging changes) suggests recurrence or progression. A >90% decline in CA 19-9 after resection is associated with better prognosis. **Warning:** CA 19-9 can be elevated in benign conditions (pancreatitis, cirrhosis, cholangitis), so it is not diagnostic alone—it must be interpreted with imaging and clinical context. 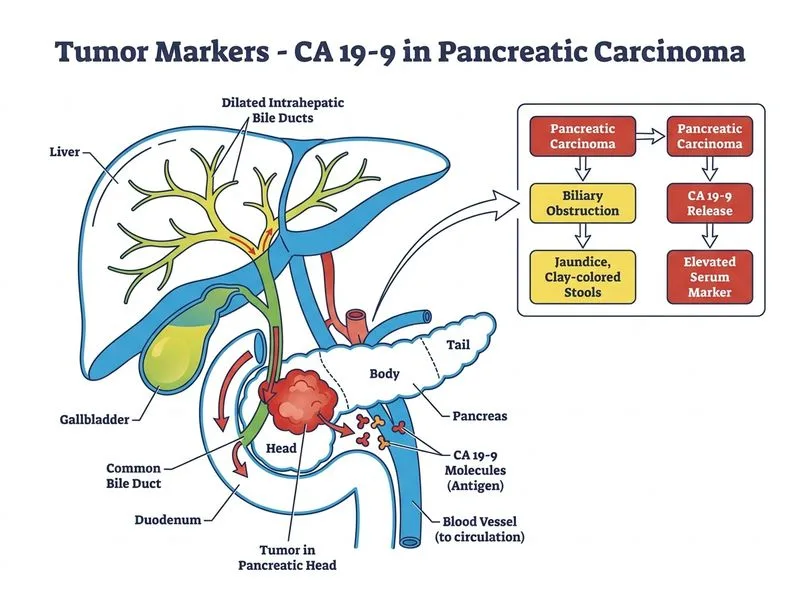
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.