## Clinical Context The patient presents with features of gestational trophoblastic neoplasia (GTN), specifically invasive mole or choriocarcinoma: persistent vaginal bleeding, pelvic mass with myometrial invasion, markedly elevated β-hCG, and elevated LDH. These findings are pathognomonic for GTN. ## β-hCG as the Primary Tumor Marker for GTN **Key Point:** β-hCG (beta human chorionic gonadotropin) is the gold standard tumor marker for gestational trophoblastic neoplasia. It is: - Produced by trophoblastic tissue (both benign and malignant) - Highly sensitive and specific for GTN - Used for diagnosis, risk stratification, and monitoring treatment response - The most reliable indicator of disease burden and treatment efficacy **High-Yield:** β-hCG has a short half-life of 24–36 hours. A falling β-hCG level during treatment indicates response; a plateau or rising level suggests treatment failure or recurrence. Complete normalization of β-hCG is required for cure and must be maintained for 3 consecutive months before treatment is stopped. ## Prognostic Significance of β-hCG in GTN | β-hCG Level | Risk Category | Prognosis | |-------------|---------------|----------| | <1,000 mIU/mL | Low risk | Excellent (>95% cure with single-agent chemotherapy) | | 1,000–10,000 mIU/mL | Low risk | Excellent | | >10,000 mIU/mL | High risk | Requires multi-agent chemotherapy; lower cure rate | | >100,000 mIU/mL | Very high risk | Aggressive disease; highest mortality risk | **Clinical Pearl:** In this patient, β-hCG of 45,000 mIU/mL places her in the high-risk category. Combined with elevated LDH (indicating high tumor burden), this patient requires multi-agent chemotherapy (typically EMA-CO regimen). β-hCG should be monitored weekly during treatment; a >10% decline per week indicates good response. **Mnemonic for GTN Monitoring:** **BHCG** = **B**est marker, **H**igh sensitivity, **C**ure confirmation, **G**old standard. β-hCG is the only tumor marker needed for GTN management. ## Why Other Markers Are Inappropriate **Warning:** Do not confuse GTN with other malignancies: - AFP is elevated in germ cell tumors (yolk sac tumors, embryonal carcinomas) and hepatocellular carcinoma, NOT in GTN - CEA is non-specific and not used in GTN - CA-125 may be mildly elevated in GTN but is not specific or prognostically useful 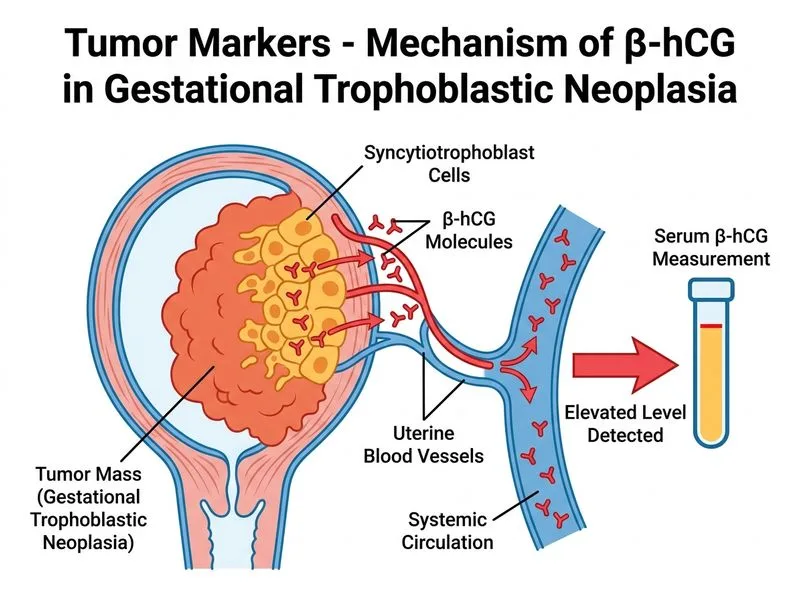
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.