Vasculitis Syndromes MCQ — NEET PG Practice Question | NEETPGAI
Vasculitis Syndromes
medium
microscope Pathology
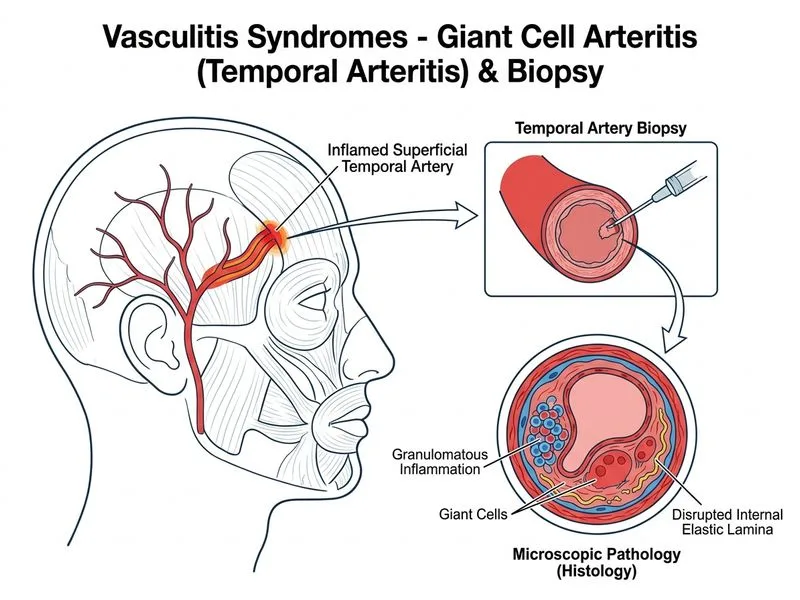
A 58-year-old man presents with sudden onset of severe headache, jaw claudication, and visual disturbances. ESR is markedly elevated at 95 mm/hr. Temporal artery palpation reveals a tender, non-pulsatile vessel. Which investigation is most appropriate to confirm the diagnosis?
A. Temporal artery biopsy
B. CT angiography of head and neck vessels
C. Serum IL-6 and CRP levels
D. Doppler ultrasound of temporal artery
Explanation
Diagnosis: Giant Cell (Temporal) Arteritis
Key Point
Temporal artery biopsy remains the gold standard confirmatory test for giant cell arteritis (GCA), demonstrating granulomatous inflammation with giant cells and intimal proliferation.
Clinical Presentation
The patient presents with classic features of GCA:
Temporal headache (most common symptom)
Jaw claudication (pathognomonic)
Visual symptoms (risk of irreversible blindness)
Markedly elevated ESR (typically >50 mm/hr)
Tender temporal artery on examination
Why Temporal Artery Biopsy is the Gold Standard
Table
Feature
Temporal Artery Biopsy
Other Investigations
Sensitivity
80–95% (gold standard)
Doppler: 60–80%
Specificity
100%
Imaging: Non-specific
Diagnostic certainty
Definitive histology
Suggestive only
Timing
Within 1–2 weeks of symptom onset
Can be delayed
Clinical impact
Confirms diagnosis, guides long-term therapy
Guides initial suspicion
High-YieldNEET PG
A positive biopsy showing granulomatous inflammation with giant cells is pathognomonic for GCA. The biopsy should be performed within 1–2 weeks of symptom onset; longer delays reduce sensitivity due to skip lesions and healing.
Biopsy Findings in GCA
1.
Granulomatous inflammation of the media and adventitia
2.
Giant cells (often at the internal elastic lamina)
3.
Intimal proliferation and luminal narrowing
4.
Lymphocytic infiltration
Clinical Pearl
Treatment with corticosteroids should NOT be delayed while awaiting biopsy if clinical suspicion is high and vision is threatened. Biopsy can be performed even after initiation of therapy, as histological changes persist for weeks.
Warning
Do not confuse GCA with polymyalgia rheumatica (PMR). While PMR often accompanies GCA (10–15% of PMR cases), PMR alone does not require biopsy — it is a clinical diagnosis based on elevated ESR and response to low-dose corticosteroids.
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.