A 42-year-old woman from Mumbai presents with a 6-week history of fever, arthralgia, and a palpable purpura rash on the lower extremities and buttocks. Urinalysis shows hematuria and mild proteinuria. Serum creatinine is 1.2 mg/dL. Skin biopsy shows IgA-dominant immune complex deposition. What is the most appropriate next step in management?
A. Start supportive care with NSAIDs and observe for 4 weeks with repeat urinalysis
B. Initiate high-dose prednisolone (1 mg/kg/day) and cyclophosphamide immediately
C. Administer intravenous immunoglobulin (IVIG) as first-line therapy
D. Perform renal biopsy to assess glomerular involvement and guide therapy
Explanation
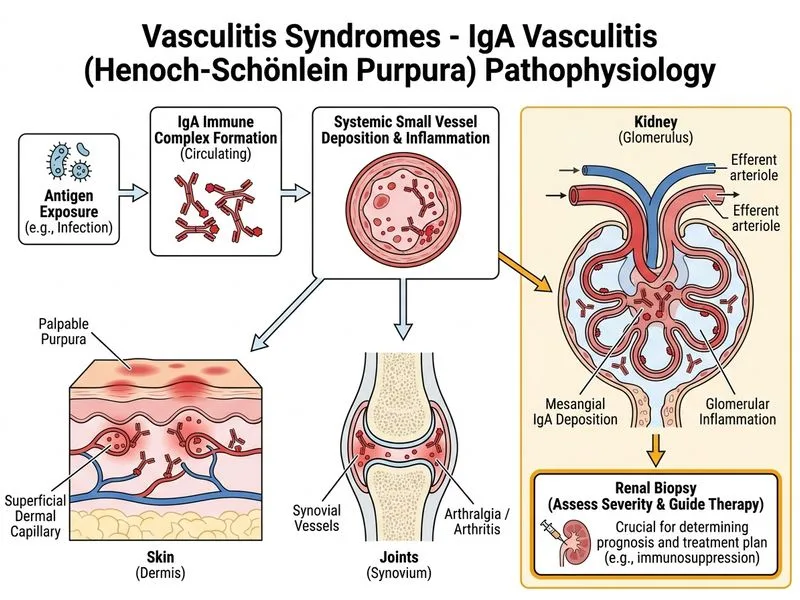
Clinical Diagnosis: IgA Vasculitis (IgAV, formerly IgA Nephropathy Vasculitis)
The presentation is classic: palpable purpura (lower extremities and buttocks), arthralgia, hematuria with proteinuria, and IgA-dominant immune complex deposition on skin biopsy.
Management Strategy: Risk Stratification via Renal Biopsy
Key Point
IgA vasculitis has variable renal involvement (from asymptomatic hematuria to rapidly progressive glomerulonephritis). Renal biopsy is essential to determine prognosis and guide intensity of immunosuppressive therapy.
High-YieldNEET PG
The presence of hematuria + proteinuria + elevated creatinine (even mild) mandates renal biopsy to assess:
Histological grade (MEST-C score)
Extent of glomerular, interstitial, and vascular involvement
Presence of crescents (indicator of aggressive disease)
Why Renal Biopsy Is the Next Step
1.
Risk stratification: MEST-C scoring predicts progression to ESRD
M (mesangial): proliferation grade
E (endocapillary): proliferation
S (segmental): sclerosis
T (tubular): atrophy
C (crescents): percentage
2.
Treatment tailoring:
Low-risk disease (no crescents, minimal proteinuria): supportive care ± corticosteroids
Baseline assessment: Establishes degree of chronicity and reversibility
Clinical Pearl
In IgAV with renal involvement, the histological findings, not just clinical presentation, determine prognosis. A patient with mild clinical signs may have crescentic disease on biopsy requiring aggressive therapy.
Management Algorithm Post-Biopsy
Loading diagram...
Supportive Measures (All Patients):
ACE inhibitor or ARB (renoprotective)
Blood pressure control (target <130/80 mmHg)
NSAID use should be minimized (risk of acute kidney injury)
Dietary sodium and protein restriction if proteinuria >1 g/day
Robbins 10e Ch 11; Harrison 21e Ch 319
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.