## Clinical Presentation & Diagnosis This patient presents with the hallmark features of **Takayasu arteritis (TA)**: a young to middle-aged woman from an endemic region (Asia, particularly India) with progressive claudication, aortic wall thickening, and markedly elevated inflammatory markers. ### Key Diagnostic Features of Takayasu Arteritis **High-Yield:** Takayasu arteritis is the classic **large-vessel vasculitis in young women from Asia**. The mnemonic is **"Pulseless disease"** — but this patient has diminished pulses, which is the early phase. **Key Point:** TA affects the aorta and its major branches (subclavian, carotid, renal, iliac arteries). The disease progresses through phases: | Phase | Features | Imaging | | --- | --- | --- | | **Early (Acute)** | Systemic inflammation, fever, arthralgia, elevated ESR/CRP | Aortic wall thickening, edema | | **Late (Chronic)** | Claudication, absent pulses, aortic regurgitation | Aortic narrowing, stenosis, occlusion | This patient is in the **late chronic phase** with aortic narrowing and claudication. ### Pathophysiology TA is a **granulomatous large-vessel vasculitis** of unknown etiology, characterized by: 1. Infiltration of the aortic media and adventitia by lymphocytes, macrophages, and granulomas 2. Progressive intimal proliferation → luminal narrowing 3. Weakening of the arterial wall → aneurysm formation (in some patients) **Clinical Pearl:** The disease is more common in women (8:1 female-to-male ratio) and typically presents in the 2nd–3rd decade, though this patient is 52 — late-onset TA is recognized. ### Why This Patient Has Takayasu Arteritis 1. **Demographics**: Young-to-middle-aged woman from India (endemic region) 2. **Large-vessel involvement**: Aortic thickening and narrowing on imaging — pathognomonic for large-vessel vasculitis 3. **Claudication + diminished femoral pulses**: Suggests aortoiliac involvement 4. **Elevated inflammatory markers (ESR 78, CRP 12)**: Indicates active inflammation 5. **Systemic hypertension**: Due to renal artery involvement (common in TA) 6. **Absence of upper respiratory tract symptoms**: Rules out GPA ### Diagnostic Criteria (Modified from American College of Rheumatology) TA diagnosis requires 3 of 6 criteria: - Age of onset < 40 years (or < 50 for late-onset) - Claudication of limbs - Decreased brachial artery pulse - BP difference > 10 mmHg between arms - Aortic brruit on auscultation - Abnormality on aortography (narrowing, occlusion, aneurysm) This patient meets multiple criteria. ### Imaging Findings in Takayasu Arteritis ```mermaid flowchart TD A[Takayasu Arteritis]:::outcome --> B[Aorta & Major Branches]:::outcome B --> C[Aortic Wall Thickening<br/>Edema & Inflammation]:::action C --> D[Progressive Luminal Narrowing<br/>Stenosis]:::action D --> E[Claudication<br/>Diminished Pulses<br/>Aortic Regurgitation]:::outcome B --> F[Aneurysm Formation<br/>Rupture Risk]:::urgent G[Imaging: CT/MRI] --> H{Findings}:::decision H -->|Early| I[Aortic wall thickening<br/>Edema]:::outcome H -->|Late| J[Luminal narrowing<br/>Stenosis<br/>Occlusion]:::outcome ``` **Mnemonic:** **TAKAYASU = Aorta + Young Asian Woman + Pulseless (late) or Diminished Pulses (early)** ### Differential Diagnosis: Large-Vessel Vasculitis | Feature | Takayasu | Giant Cell Arteritis | Atherosclerosis | | --- | --- | --- | --- | | **Age of onset** | < 40 (or < 50) | > 50 | > 50 | | **Gender** | Female predominance (8:1) | Female predominance | Male > Female | | **Vessels affected** | Aorta + major branches | Temporal, carotid, aorta | Coronary, cerebral, peripheral | | **ESR** | Markedly elevated | Markedly elevated (> 50) | Normal | | **Histology** | Granulomatous inflammation | Granulomatous inflammation | Lipid-laden macrophages | | **Temporal artery biopsy** | Not involved | **Diagnostic** | Not applicable | | **Geography** | Asia, Latin America | Caucasian, > 50 years | Universal | **Clinical Pearl:** Both TA and GCA are granulomatous large-vessel vasculitides with elevated inflammatory markers, but **age and geography are the key discriminators**. TA is young Asian women; GCA is elderly Caucasians. Temporal artery involvement is pathognomonic for GCA, not TA. ### Management 1. **Corticosteroids**: First-line therapy (prednisolone 1 mg/kg/day, then taper) 2. **Immunosuppressants**: Methotrexate or azathioprine for steroid-sparing effect 3. **Antiplatelet therapy**: Aspirin to reduce thrombotic complications 4. **Surgical intervention**: Bypass grafting or angioplasty for critical stenosis [cite:Robbins 10e Ch 20; Harrison 21e Ch 328] 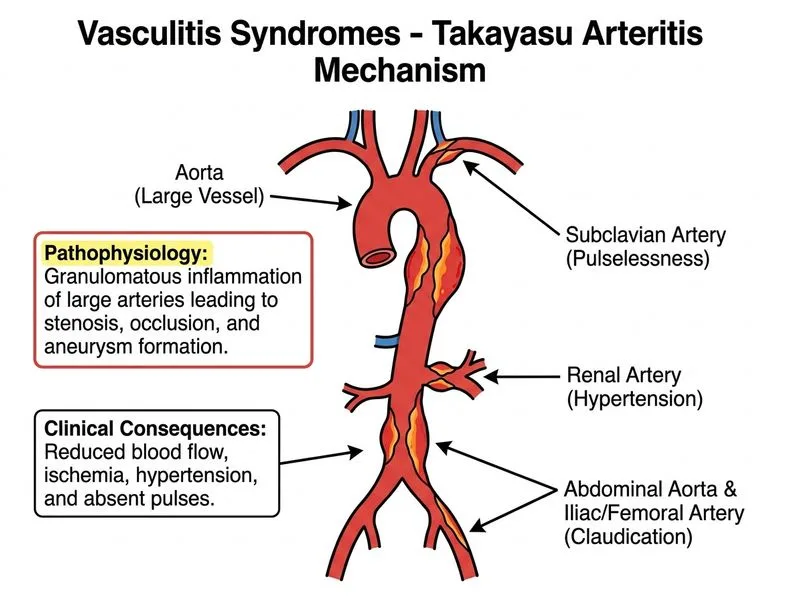
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.