Viral Keratitis MCQ — NEET PG Practice Question | NEETPGAI
Viral Keratitis
medium
eye Ophthalmology
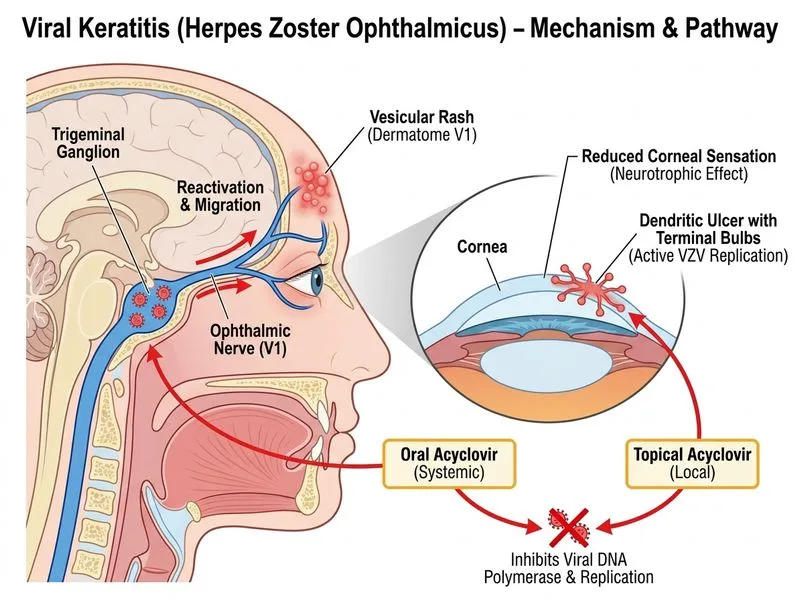
A 32-year-old woman presents with a 5-day history of right eye pain, photophobia, and blurred vision. She reports a vesicular rash on the forehead and upper eyelid 2 days prior to eye symptoms. On examination, visual acuity is 6/9, and slit-lamp biomicroscopy reveals branching dendritic ulcers with terminal bulbs on the cornea. Corneal sensation is reduced. What is the most appropriate initial pharmacological management?
A. Topical interferon-alpha 6 times daily plus oral ribavirin
B. Topical cidofovir 1% 4 times daily for 3 weeks
C. Topical acyclovir 5 times daily plus oral acyclovir 400 mg 5 times daily for 10 days
D. Topical ganciclovir 5 times daily for 2 weeks
Explanation
Clinical Diagnosis
Key Point
The constellation of vesicular rash on V1 distribution (forehead/eyelid), dendritic ulcers with terminal bulbs, and reduced corneal sensation is pathognomonic for Herpes Simplex Virus (HSV) keratitis, specifically primary HSV-1 infection.
Mechanism of Dendritic Ulcers
Dendritic ulcers in HSV keratitis result from viral replication in corneal epithelial cells. The characteristic branching pattern with terminal bulbs represents:
Central area of infected epithelial cells (staining with rose bengal or lissamine green)
Lateral extensions of viral spread along nerve endings
Terminal bulbs at the tips of dendrites (areas of active viral replication)
Management Algorithm
Loading diagram...
Pharmacological Rationale
Table
Agent
Indication
Mechanism
Notes
Topical Acyclovir 5%
Epithelial HSV keratitis (dendritic/geographic)
Viral DNA polymerase inhibitor; high corneal penetration
First-line for epithelial disease
Oral Acyclovir 400 mg 5×/day
Systemic viral suppression
Achieves therapeutic aqueous humor levels
Reduces recurrence risk; essential in primary infection
Topical Ganciclovir
CMV keratitis (rare in immunocompetent)
Broader spectrum; requires phosphorylation by viral kinase
Not first-line for HSV; reserved for acyclovir resistance
Topical Cidofovir
Acyclovir-resistant HSV (immunocompromised)
Nucleotide analog; direct viral DNA inhibition
Expensive; reserved for resistant cases
Interferon-alpha
Adjunctive in severe stromal disease
Antiviral + immunomodulatory
Rarely used as monotherapy; outdated
High-YieldNEET PG
Combination of topical acyclovir 5 times daily + oral acyclovir 400 mg 5 times daily is the gold standard for primary HSV epithelial keratitis. Oral therapy reduces systemic viral load and prevents contralateral eye involvement and recurrences.
Clinical Pearls
Clinical Pearl
Reduced corneal sensation in HSV keratitis is due to viral invasion of trigeminal nerve terminals and is a hallmark finding that distinguishes HSV from bacterial keratitis.
Warning
Do NOT use topical steroids in epithelial HSV keratitis — they promote geographic ulceration (coalescence of dendrites). Steroids are only indicated in stromal or endothelial disease, always with concurrent antiviral cover.
Key Point
The dendritic ulcer typically heals within 7–10 days with appropriate antiviral therapy. Failure to heal suggests acyclovir resistance (rare in immunocompetent hosts) or incorrect diagnosis.
Expected Course
1.
Epithelial healing: 7–10 days with topical + oral acyclovir
2.
Corneal sensation recovery: weeks to months
3.
Recurrence rate: 50% within 5 years (oral prophylaxis reduces to 20%)
Loading illustration…
Practice similar questions
Sign up free to access AI-powered MCQ practice with detailed explanations and adaptive learning.