autonomic pharmacology
cholinergic
adrenergic
organophosphate poisoning
atropine
Pharmacology
NEET PG 2026
Master cholinergic and adrenergic agonists/antagonists, receptor subtypes, OP poisoning and India pesticide context with NEET PG 2026 pharmacology MCQ traps.
Autonomic pharmacology is a 3 to 5 question topic per NEET PG paper. Lock these:
Autonomic pharmacology is the highest-volume topic on the pharmacology paper and the busiest overlap with internal medicine (CHF, HTN, asthma, COPD, glaucoma, BPH), psychiatry (ADHD, PTSD nightmares), and forensic medicine (OP suicide — accounting for ~one-third of all suicide deaths in India). Lock the receptor → signalling → drug → indication → adverse effect chain for every class and you have a high-yield 4 to 6 question domain locked.
This NEETPGAI deep dive covers cholinergic agonists/antagonists, adrenergic agonists/antagonists, the receptor coupling table, organophosphate poisoning (India context), and the high-yield MCQ traps. Pair this with the GI physiology guide for ANS control of GI smooth muscle.
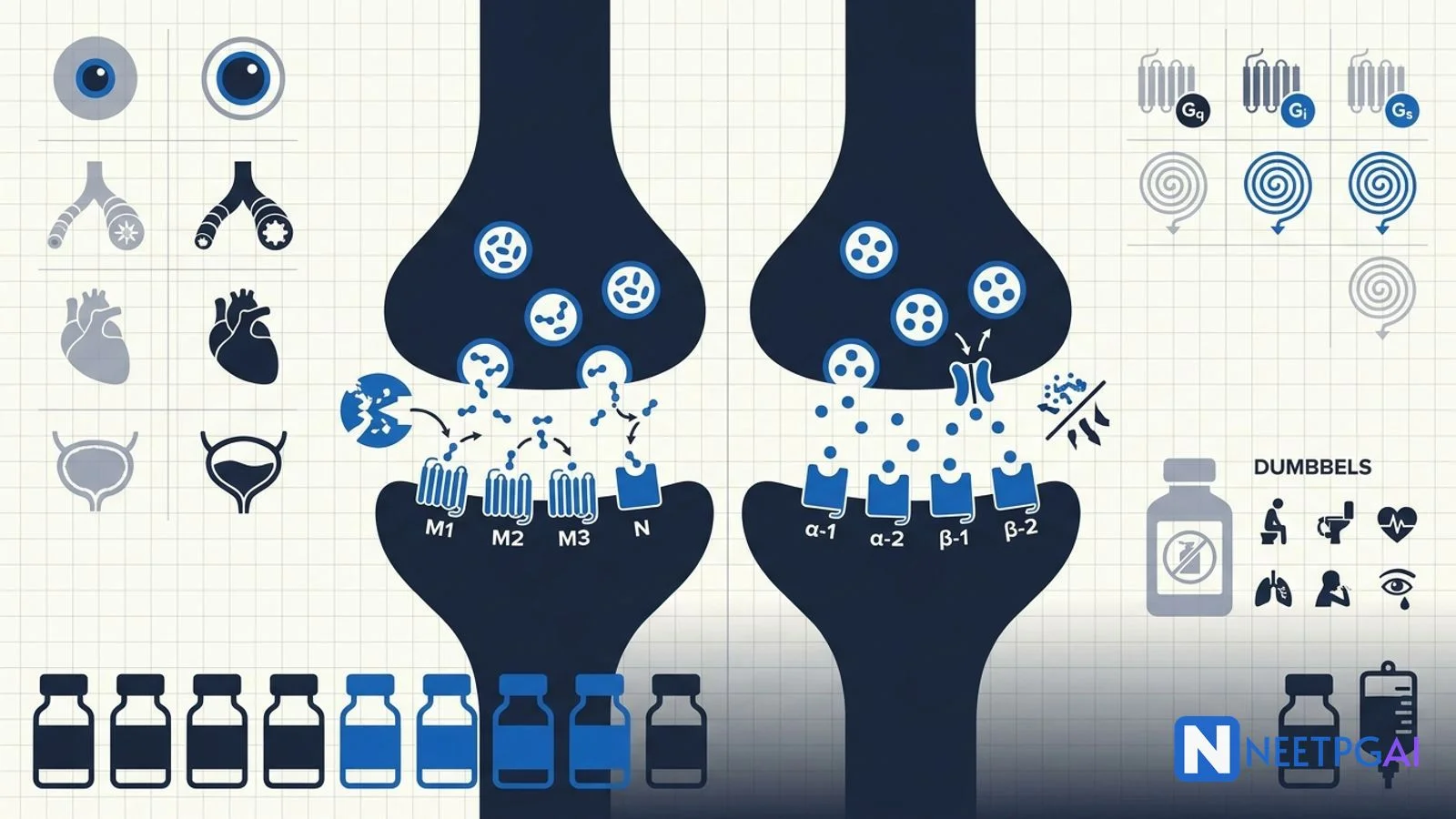
| Receptor | G-protein | Second messenger | Major location |
|---|---|---|---|
| M1 | Gq | IP3, DAG, Ca2+ | CNS, gastric parietal cell |
| M2 | Gi | ↓ cAMP | Cardiac (SA, AV node) |
| M3 | Gq | IP3, DAG, Ca2+ | Smooth muscle, glands |
| M5 | Gq | IP3, DAG | CNS |
| Nicotinic-N (Nn) | Ligand-gated cation | — | Autonomic ganglia, adrenal medulla |
| Nicotinic-M (Nm) | Ligand-gated cation | — | Skeletal muscle NMJ |
| Alpha-1 | Gq | IP3, DAG | Vascular smooth muscle, prostate, bladder neck |
| Alpha-2 | Gi | ↓ cAMP | Presynaptic CNS/sympathetic (negative feedback), pancreatic beta cell |
| Beta-1 |
Start practicing INI-CET MCQs with AI-powered explanations.
Start Free PracticeMaster GI secretions, digestion, absorption transporters, motility patterns, and gut hormones with high-yield NEET PG 2026 traps and India-context examples.
Master labor stages, Friedman vs Zhang curves, WHO partograph, AMTSL, episiotomy and India JSY/LaQshya policies for NEET PG 2026 OBG MCQs.
5 anterior segment ophthalmology image MCQs for NEET PG: hypopyon and Behcet, Kayser-Fleischer ring in Wilson, Brushfield spots in Down, corneal arcus, and pterygium vs pinguecula.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →| Gs |
| ↑ cAMP |
| Heart (SA, AV, ventricle), JGA (renin) |
| Beta-2 | Gs | ↑ cAMP | Bronchi, uterus, skeletal-muscle vasculature, liver |
| Beta-3 | Gs | ↑ cAMP | Adipose tissue (lipolysis), bladder detrusor |
| D1 | Gs | ↑ cAMP | Renal arterioles, smooth muscle |
| D2 | Gi | ↓ cAMP | Nigrostriatal, pituitary (inhibits prolactin) |
Mnemonic for Gq: "HAVe 1 M&M" — H1, Alpha-1, V1, M1, M3.
| Drug | Duration | Major use |
|---|---|---|
| Edrophonium | Ultra-short | Old Tensilon test (now obsolete) |
| Neostigmine | Short | Reversal of non-depolarising NMB; myasthenia gravis (with glycopyrrolate to block muscarinic effects) |
| Pyridostigmine | Long (4 to 6 h) | Myasthenia gravis chronic therapy |
| Physostigmine | Crosses BBB | Atropine poisoning, glaucoma (rare) |
| Donepezil, rivastigmine, galantamine | Long | Alzheimer disease |
| Organophosphates (parathion, malathion, sarin) | Irreversible | Pesticides, nerve agents — toxicology only |
"Hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter, full as a flask" — hyperthermia, anhidrosis, flushing, mydriasis, delirium, urinary retention. Treat with physostigmine (crosses BBB).
Organophosphates and carbamates are irreversible AChE inhibitors. They cause both muscarinic and nicotinic features.
Clinical + low red-cell or plasma cholinesterase. Reduced plasma butyrylcholinesterase is more sensitive but less specific.
Carbamates (e.g., physostigmine, pyridostigmine, carbaryl) cause similar features but are reversible — atropine alone is usually sufficient; pralidoxime is NOT routinely given.
India accounts for about one-third of global OP suicide deaths (~50,000 to 60,000 per year), driven by agrarian distress and easy household pesticide access. Ban of WHO Class I OPs (parathion, methyl parathion, monocrotophos) and rollout of safer storage practices are public-health priorities.
| Drug | Receptor | Use |
|---|---|---|
| Phenylephrine | Alpha-1 | Decongestant, hypotension |
| Clonidine, methyldopa, dexmedetomidine | Alpha-2 (central) | HTN, opioid withdrawal, sedation; methyldopa in pregnancy |
| Dobutamine | Beta-1 | Cardiogenic shock, stress echo |
| Salbutamol, terbutaline | Beta-2 | Acute asthma, tocolysis |
| Salmeterol, formoterol | Long-acting beta-2 | COPD, asthma maintenance |
| Mirabegron | Beta-3 | Overactive bladder |
| Drug | Selectivity | Notes |
|---|---|---|
| Atenolol, metoprolol, bisoprolol | Beta-1 selective | HTN, post-MI, CHF (bisoprolol) |
| Esmolol | Beta-1, ultra short-acting | IV intra-op |
| Nebivolol | Beta-1 + vasodilation (NO release) | HTN with metabolic benefit |
| Propranolol | Non-selective | Migraine prophylaxis, essential tremor, thyrotoxicosis, anxiety, portal HTN |
| Timolol | Non-selective | Topical for glaucoma |
| Sotalol | Non-selective + Class III antiarrhythmic | Refractory arrhythmias |
| Carvedilol | Alpha-1 + non-selective beta | Heart failure |
| Labetalol | Alpha-1 + non-selective beta | Hypertensive emergency, pregnancy HTN |
Phenoxybenzamine (alpha-blockade) FIRST for 10 to 14 days, THEN beta-blocker. If beta blocked first, unopposed alpha causes hypertensive crisis.
Direct cholinergic agonists bind muscarinic or nicotinic receptors directly — pilocarpine (M, glaucoma), bethanechol (M, urinary retention), methacholine (M, asthma challenge testing), nicotine, varenicline. Indirect cholinergic agonists are acetylcholinesterase inhibitors — they raise endogenous ACh by blocking its breakdown. Examples include neostigmine and pyridostigmine for myasthenia gravis, edrophonium (short-acting; old Tensilon test), donepezil/rivastigmine/galantamine for Alzheimer disease, and the organophosphates (irreversible AChE inhibitors used as pesticides and nerve agents).
Organophosphate poisoning causes cholinergic crisis from irreversible inhibition of acetylcholinesterase (DUMBBELS muscarinic + nicotinic features). Management — (1) decontaminate clothes/skin, ABC + intubation if respiratory failure; (2) atropine titrated to drying of secretions and clear lungs (start 2 to 4 mg IV, double every 5 minutes until atropinised); (3) pralidoxime (2-PAM) 1 to 2 g IV over 30 minutes within 24 hours, before 'ageing' of the enzyme-OP complex; (4) supportive care + ventilation. India accounts for about one-third of global OP suicide deaths.
Beta-1 selective ('cardioselective') — atenolol, metoprolol, bisoprolol, esmolol (ultra short-acting IV), nebivolol. Non-selective — propranolol, nadolol, timolol, sotalol. Beta + alpha-1 — carvedilol (heart failure), labetalol (hypertensive emergency, pregnancy). Selectivity is dose-dependent; at high doses cardioselective agents also block beta-2. Nebivolol is unique in having vasodilatory NO-releasing activity. Sotalol has class III antiarrhythmic activity (K+ channel block). Beta-blockers reduce mortality in heart failure, post-MI, and arrhythmias.
Clonidine is a central alpha-2 adrenergic agonist that activates presynaptic alpha-2 receptors in the rostral ventrolateral medulla, reducing sympathetic outflow and lowering blood pressure, heart rate, and noradrenaline release. Uses include hypertension (especially urgency), opioid and alcohol withdrawal (suppresses sympathetic surge), ADHD, hot flushes, and as an anaesthesia adjunct (sedation + analgesia). Side effects — sedation, dry mouth, bradycardia, and rebound hypertension on abrupt withdrawal (taper required). Dexmedetomidine is a more selective alpha-2 agonist used for ICU sedation.
Alpha-1 antagonists block postsynaptic alpha-1 receptors on vascular smooth muscle (vasodilation), bladder neck and prostate (relaxation). Non-selective alpha (phenoxybenzamine — irreversible, long-acting) is used preoperatively for pheochromocytoma. Selective alpha-1 antagonists are used for benign prostatic hyperplasia (tamsulosin and silodosin are uroselective for alpha-1A on prostate; less postural hypotension than terazosin or doxazosin). Prazosin is used for PTSD nightmares and resistant hypertension. First-dose hypotension is a class effect.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026