Fungal Infections — Dermatomycosis to Systemic for NEET PG 2026
Master dermatophytes, candida, mucormycosis, cryptococcus, histoplasma, aspergillus and post-COVID black fungus with India-specific antifungal stewardship for NEET PG 2026.
Dr. NEETPGAI Editorial TeamPublished 25 May 202615 min read
Share this article
Ready to put this into practice?
Start practicing NEET PG MCQs with AI-powered explanations.
PCP — TMP-SMX plus steroids if hypoxia; CD4 driven HIV prophylaxis.
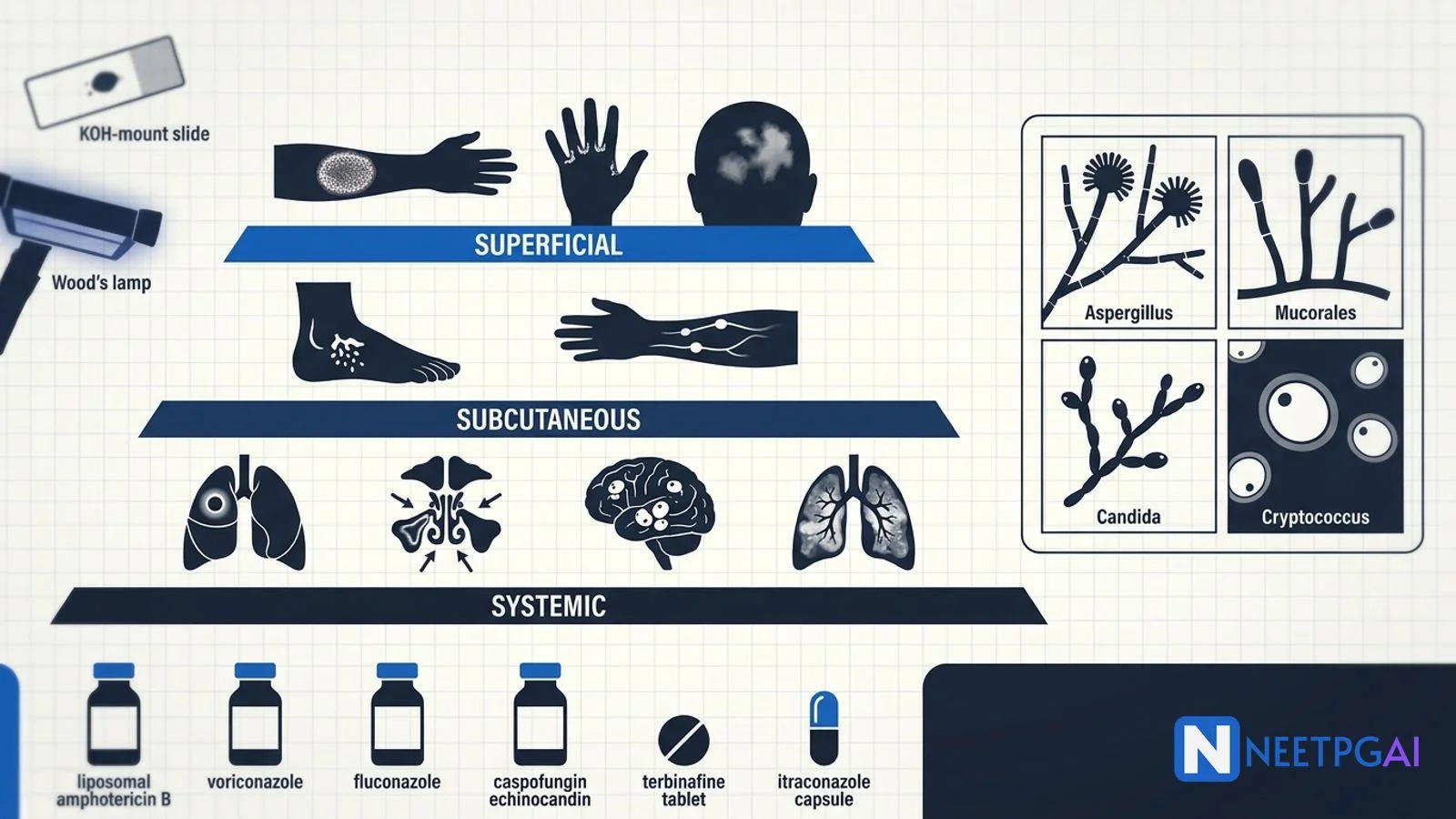
Fungal infections have become disproportionately important on NEET PG since the post-COVID mucormycosis epidemic (2021) and the parallel global emergence of antifungal-resistant Candida auris. The dermatophyte epidemic in India — driven by widespread topical steroid abuse and the rise of antifungal-resistant T. mentagrophytes Type VIII — has changed first-line therapy recommendations. Vignettes increasingly require you to read the host (HIV, post-transplant, diabetic, post-COVID), the site (skin, lung, CNS, sinus), and the morphology (hyphal width, septation, branching angle) and pick the right antifungal.
This NEETPGAI deep dive walks through the systematic classification (superficial, subcutaneous, systemic), key clinical syndromes, KOH and histopathology features, and the antifungal armamentarium with India-specific stewardship issues. Pair this with the leprosy classification and MDT guide and the otitis media and sinusitis ENT guide for the full mycobacterial and ENT-fungal coverage.
Distal-lateral subungual onychomycosis commonest; nail thickening, discolouration
Face
Tinea faciei
Often misdiagnosed as eczema
Hands
Tinea manuum
Usually unilateral, "two feet one hand syndrome"
Diagnosis:
KOH mount — dissolves keratin; reveals septate hyphae and arthroconidia under microscope.
Wood's lamp — green fluorescence in Microsporum (canis, audouinii) and T. schoenleinii (favus). NOT useful for the current Indian T. mentagrophytes and T. rubrum epidemics.
Culture — Sabouraud dextrose agar at 25 degrees C; takes 3 to 4 weeks; identifies species and antifungal susceptibility.
Oral griseofulvin — first-line for tinea capitis (children); 20 to 25 mg/kg/day for 6 to 8 weeks.
AVOID topical steroids — combination topical steroid-antifungal creams (clobetasol-clotrimazole sold over the counter in India) have driven the current T. mentagrophytes Type VIII epidemic by suppressing immune clearance.
Candida infections
Yeast that buds; commensal in mouth, gut, vagina and skin folds.
Common clinical patterns:
Oral thrush (pseudomembranous candidiasis) — white plaques that scrape off easily; immunosuppression, denture-wearers, infants, HIV (CD4 under 200).
Vulvovaginal candidiasis — cheesy white discharge, pruritus; common in diabetes and pregnancy.
Intertrigo — beefy red plaques in skin folds with satellite pustules; obese diabetics.
Diaper candidiasis — erythematous plaques with satellite pustules in the napkin area.
Candidaemia and disseminated candidiasis — bloodstream invasion in ICU patients with central lines, broad-spectrum antibiotics, or neutropenia.
Diagnosis — KOH mount shows yeast cells with budding (blastoconidia) and pseudohyphae; culture on Sabouraud; serum 1,3-beta-D-glucan for invasive disease.
Treatment:
Mucocutaneous — topical clotrimazole or nystatin for oral thrush; oral fluconazole 150 mg single dose for vaginal candidiasis.
Candidaemia — echinocandin (caspofungin, micafungin, anidulafungin) for 14 days after first negative culture; step-down to fluconazole if susceptible.
C. auris (rising in India) — multidrug-resistant Candida species first described in 2009; high mortality; resistant to fluconazole, often amphotericin and echinocandins; isolation, infection control, and echinocandins as initial empirical choice.
Pityriasis versicolor
Superficial infection caused by lipophilic yeast Malassezia furfur (formerly Pityrosporum). Hypopigmented or hyperpigmented coalescing patches over upper trunk, neck and arms; fine scale on scratching.
KOH mount — "spaghetti-and-meatballs" appearance (short hyphae plus round yeast clusters).
Wood's lamp — yellowish fluorescence in some cases.
Treatment — topical selenium sulphide, ketoconazole shampoo, or topical terbinafine; oral fluconazole or itraconazole for extensive disease. Pigmentary changes can take months to resolve.
Subcutaneous fungal infections
Mycetoma (Madura foot)
Chronic suppurative granulomatous disease following traumatic inoculation (barefoot walking, thorn injury) — endemic in tropical India (Tamil Nadu, Rajasthan, Maharashtra) and northern Africa.
Eumycetoma — caused by fungi (Madurella mycetomatis, Pseudallescheria boydii); black grains discharged through sinuses.
Actinomycetoma — caused by actinomycetes bacteria (Nocardia, Actinomadura, Streptomyces); white, yellow or red grains.
Classic triad — chronic swelling, multiple sinuses, grains in discharge. Foot is the commonest site (over 80 percent). Treatment differs — eumycetoma needs prolonged itraconazole or voriconazole and surgery; actinomycetoma responds to cotrimoxazole or dapsone.
Sporotrichosis ("rose gardener's disease")
Caused by Sporothrix schenckii — dimorphic fungus inoculated through skin (rose thorn, soil). Forms a primary lesion at the site of inoculation that ulcerates, then characteristic linear chain of nodules along lymphatic vessels.
Treatment — itraconazole 200 mg daily for 3 to 6 months; saturated potassium iodide is older traditional treatment.
Chromoblastomycosis
Slowly progressive verrucous (warty), violaceous, cauliflower-like plaque on a lower limb after traumatic implantation of pigmented (dematiaceous) fungi (Fonsecaea pedrosoi). Histology shows characteristic sclerotic (medlar / copper-penny) bodies.
Systemic (deep) mycoses
Cryptococcosis
Caused by Cryptococcus neoformans (var. grubii, gattii) — encapsulated yeast acquired by inhalation of pigeon droppings or soil.
HIV-defining illness when CD4 under 100 cells/microL; also affects organ transplant recipients and patients on long-term steroids.
Diagnosis — India ink CSF stain shows the thick polysaccharide capsule (clear halo around yeast); cryptococcal capsular antigen (CrAg) on CSF and serum (latex agglutination or lateral flow assay — over 95 percent sensitive); culture on Sabouraud.
Treatment — induction with liposomal amphotericin B (3 to 4 mg/kg/day) plus 5-flucytosine (100 mg/kg/day) for 2 weeks, consolidation with fluconazole 800 mg/day for 8 weeks, then maintenance fluconazole 200 mg/day until CD4 over 100 for 6 months.
Histoplasmosis
Caused by Histoplasma capsulatum — dimorphic fungus endemic in river valleys (Mississippi-Ohio in the US, Ganges valley in India), bat caves, and bird droppings.
Asymptomatic primary infection in immunocompetent — calcified granulomas on chest X-ray mimic TB.
Acute pulmonary histoplasmosis — flu-like illness with mediastinal lymphadenopathy.
Disseminated in HIV — fever, hepatosplenomegaly, mucocutaneous ulcers, marrow involvement.
Diagnosis — urinary Histoplasma antigen (most sensitive in disseminated disease), serum antigen, bone marrow biopsy (intracellular yeasts in macrophages), culture.
Treatment — itraconazole for mild-moderate; liposomal amphotericin B then itraconazole for severe disseminated.
Aspergillosis
Caused by Aspergillus fumigatus (commonest), A. flavus, A. niger — ubiquitous filamentous mould.
Surgical resection if symptomatic; voriconazole adjunct
Invasive aspergillosis
Neutropenic, transplant
Halo sign, air-crescent sign; angioinvasion
IV voriconazole; isavuconazole or liposomal amphotericin alternative
Chronic pulmonary aspergillosis
Mild immune deficit, post-TB
Progressive cavitation, fibrosis
Long-term itraconazole or voriconazole
Histology — narrow (3 to 6 micrometres) septate hyphae with acute-angle (45 degree) branching.
Mucormycosis (black fungus, zygomycosis)
Caused by Mucorales (Rhizopus, Mucor, Lichtheimia, Cunninghamella). India had the world's largest post-COVID mucormycosis epidemic in 2021 — over 51,000 cases.
Risk factors:
Uncontrolled diabetes mellitus (commonest in India).
Diabetic ketoacidosis.
Iron overload (deferoxamine therapy paradoxically promotes Mucor growth).
Cutaneous — necrotic eschar after burn, trauma, or contaminated dressings.
Gastrointestinal — neonates, malnutrition.
Disseminated — high mortality.
Diagnosis — KOH and histopathology of biopsy showing broad (10 to 20 micrometres) ASEPTATE ribbon-like hyphae with RIGHT-ANGLE (90 degree) branching. Tissue necrosis with angioinvasion is characteristic.
Treatment — liposomal amphotericin B 5 to 10 mg/kg/day IV (first-line) plus aggressive surgical debridement plus reversal of immunosuppression (insulin, stop steroids). Step-down to oral posaconazole or isavuconazole for maintenance. Mortality 30 to 50 percent despite optimal therapy.
Pneumocystis pneumonia (PCP)
Caused by Pneumocystis jirovecii (previously P. carinii, reclassified from protozoan to atypical fungus).
Hosts — HIV with CD4 under 200, chronic high-dose corticosteroids, transplant recipients, leukaemia, severe malnutrition.
Diagnosis — induced sputum or BAL with silver methenamine, Giemsa, or immunofluorescence — cup-shaped or helmet-shaped cysts; PCR.
Treatment — TMP-SMX (trimethoprim-sulfamethoxazole) 15 to 20 mg/kg/day of TMP component for 21 days. Add prednisolone 40 mg twice daily × 5 days then taper if PaO2 under 70 mmHg or A-a gradient over 35 mmHg.
Alternatives — pentamidine, atovaquone, clindamycin plus primaquine, dapsone plus TMP.
Prophylaxis — TMP-SMX 1 single-strength tablet daily for HIV with CD4 under 200; continue until CD4 over 200 for 3 consecutive months on ART.
Adjunct with amphotericin for cryptococcal meningitis
Griseofulvin
Griseofulvin
Binds tubulin, disrupts mitotic spindle
Tinea capitis (children)
Voriconazole — first-line for invasive aspergillosis; requires therapeutic drug monitoring (TDM) because of saturable metabolism and inter-individual variability; side effects include visual disturbance, hepatotoxicity, periostitis with long-term use.
Amphotericin B — significant nephrotoxicity (afferent arteriole vasoconstriction, distal tubular dysfunction with hypokalaemia, hypomagnesaemia, renal tubular acidosis); liposomal formulations are far less nephrotoxic and allow higher doses (5 to 10 mg/kg/day) for mucormycosis.
NEET PG MCQ traps
Dermatophyte genera — Trichophyton (skin, hair, nails), Microsporum (skin, hair), Epidermophyton (skin, nails — NEVER hair).
KOH mount dissolves keratin; reveals septate hyphae.
Wood's lamp — Microsporum canis/audouinii green; T. mentagrophytes NEGATIVE.
PCP — silver stain shows cup/helmet-shaped cysts; TMP-SMX first-line; add prednisolone if PaO2 under 70.
PCP prophylaxis — TMP-SMX SS daily if CD4 under 200; continue until CD4 over 200 × 3 months on ART.
Black fungus is NOT pigmented — name comes from ischaemic tissue necrosis, not fungal pigmentation.
Recent updates and Indian context
India dermatophyte epidemic — T. mentagrophytes Type VIII has driven a recalcitrant, often steroid-modified, terbinafine-resistant epidemic across India since 2015; current Indian Association of Dermatologists, Venereologists and Leprologists (IADVL) guidelines recommend itraconazole 200 mg daily for 6 to 8 weeks as first-line for extensive disease and explicitly prohibit topical steroid-antifungal combinations.
Post-COVID mucormycosis epidemic — over 51,000 cases reported during the April-July 2021 wave; ICMR mucormycosis advisory established case definitions and treatment standards; mortality 30 to 50 percent.
Candida auris emergence — first isolated in India in 2010; over 80 percent of global C. auris cases reported from Indian ICUs; AIIMS and Tata Memorial Centre now isolate suspected cases and use echinocandin empirically.
National Action Plan for Antimicrobial Resistance (NAP-AMR) — includes antifungal stewardship; restricts unmonitored sale of fluconazole, voriconazole, itraconazole.
Isavuconazole — newer triazole approved in India for invasive aspergillosis and mucormycosis; better tolerated than voriconazole.
Cryptococcal antigen screen-and-treat strategy — implemented in HIV patients with CD4 under 100 at AIIMS and major Indian HIV centres; pre-emptive fluconazole reduces meningitis incidence.
WHO Priority Pathogens Fungal List (2022) — Candida auris, Cryptococcus neoformans, Aspergillus fumigatus, Candida albicans are critical-priority pathogens; mucormycosis and histoplasmosis are high-priority.
Frequently asked questions
How do dermatophytes differ from yeasts and moulds?
Dermatophytes are keratinophilic filamentous fungi that invade non-living keratinised tissue (stratum corneum, hair, nails) and cause tinea infections. The three genera are Trichophyton (skin, hair, nails — commonest), Microsporum (skin and hair), and Epidermophyton (skin and nails, never hair). Yeasts are unicellular fungi reproducing by budding (Candida, Cryptococcus, Malassezia). Moulds are multicellular filamentous fungi with hyphae (Aspergillus, Mucorales). Dimorphic fungi (Histoplasma, Blastomyces, Coccidioides) switch between yeast in tissue and mould in culture at 25 degrees C.
What is the KOH mount and Wood's lamp role in dermatophyte diagnosis?
KOH (potassium hydroxide 10 to 20 percent) mount dissolves keratin in skin scrapings, hair or nail clippings, revealing septate fungal hyphae under microscopy within 10 to 15 minutes — the bedside gold-standard rapid test. Wood's lamp (long-wave UV at 365 nm) is used in tinea capitis — Microsporum canis and M. audouinii fluoresce bright green; T. tonsurans does NOT fluoresce; T. schoenleinii (favus) fluoresces dull green. Many India dermatophyte epidemics are T. mentagrophytes or T. rubrum, both of which are Wood's lamp negative.
Why is mucormycosis called black fungus and how is it diagnosed?
Mucormycosis is colloquially called black fungus because it causes ischaemic necrosis of the affected tissue — angioinvasion of blood vessels leads to thrombosis and infarction, producing characteristic black eschars on the palate, nasal mucosa or skin. The fungi themselves are NOT pigmented (they are pale hyaline). Diagnosis requires KOH mount and histopathology of biopsied tissue showing BROAD (10 to 20 micrometres) ASEPTATE ribbon-like hyphae with RIGHT-ANGLE branching. Aspergillus, in contrast, shows narrow (3 to 6 micrometres) septate hyphae with acute-angle (45 degree) branching.
What is the management of invasive aspergillosis?
Invasive aspergillosis presents with fever, cough, haemoptysis and pleuritic chest pain in an immunocompromised host (haematologic malignancy, prolonged neutropenia, post-transplant). CT chest shows the halo sign early (ground-glass around a nodule) and the air-crescent sign late (cavitation). Diagnosis is by serum and BAL galactomannan, beta-D-glucan, and tissue biopsy. First-line treatment is intravenous voriconazole 6 mg/kg twice on day 1 then 4 mg/kg twice daily, with therapeutic drug monitoring. Alternatives include isavuconazole, liposomal amphotericin B and posaconazole. Duration is 6 to 12 weeks, longer in refractory cases.
How is Pneumocystis jirovecii pneumonia (PCP) diagnosed and treated?
PCP affects HIV patients with CD4 under 200 cells/microL, and other severely immunocompromised hosts (chronic high-dose steroids, transplant). Presents with subacute dry cough, dyspnoea on exertion, and fever; CXR shows bilateral perihilar interstitial infiltrates; CT shows ground-glass opacities. Diagnosis is by induced sputum or BAL with silver methenamine or immunofluorescence stain — cup-shaped, helmet-shaped cysts. First-line treatment is TMP-SMX (trimethoprim-sulfamethoxazole) 15 to 20 mg/kg/day of trimethoprim component intravenously for 21 days, with adjunctive prednisolone if PaO2 under 70 mmHg or A-a gradient over 35 mmHg. HIV patients need ART and lifelong PCP prophylaxis until CD4 over 200 for 3 months.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026