Quick Answer
Leprosy contributes 2 to 3 NEET PG questions per paper across Dermatology, Microbiology, Medicine and Community Medicine — India still carries the largest absolute case burden globally. Lock these:
- Mycobacterium leprae — intracellular, acid-fast, prefers cool peripheral nerves and skin.
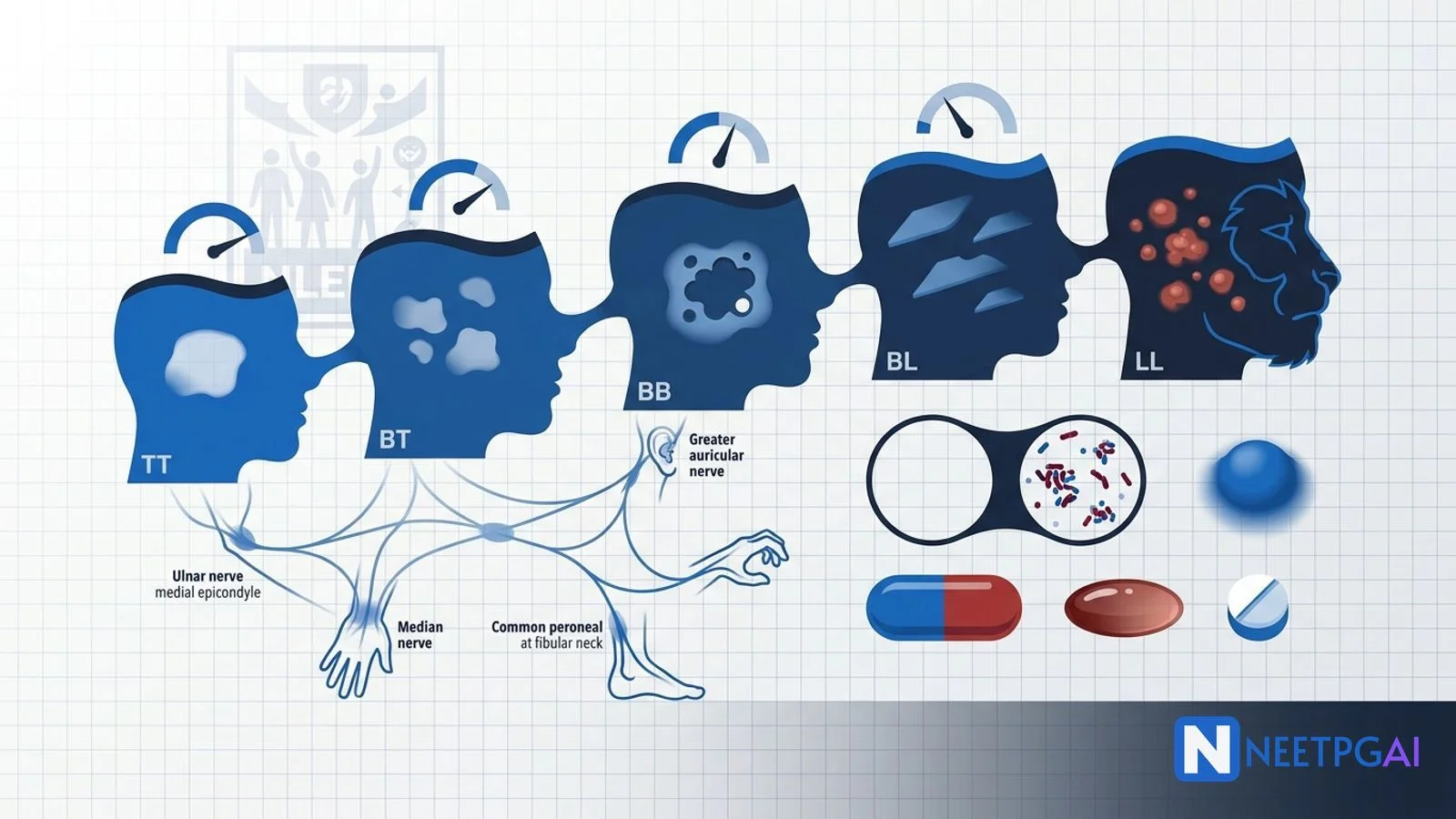
- Ridley-Jopling spectrum — TT-BT-BB-BL-LL based on CMI strength.
- WHO classification — PB (5 or fewer lesions, smear negative) vs MB (greater than 5 lesions, smear positive, multiple nerves).
- Hallmark findings — anaesthetic hypopigmented patch, thickened nerve, peripheral palsy (ulnar, median, peroneal).
- Diagnosis — slit-skin smear with Fite-Faraco stain; biopsy; bacterial and morphological index.
- WHO MDT 2018 — rifampicin + clofazimine + dapsone; PB 6 months, MB 12 months.
- Reactions — type 1 reversal (steroids), type 2 ENL (steroids, thalidomide, clofazimine).
Leprosy looks like a "post-elimination" disease but India still reports the highest annual case detection rate in the world — about 60 percent of new global cases. NEET PG and the National Leprosy Eradication Programme (NLEP) curricula expect you to read a clinical vignette and immediately classify, treat and manage reactions and disability. The exam loves the immunological spectrum, the slit-skin smear interpretation and the type 1 vs type 2 reaction trap.
This NEETPGAI deep dive walks through M. leprae biology, the Ridley-Jopling and WHO classifications, slit-skin smear technique, the lepromin test, WHO MDT, type 1 and type 2 lepra reactions, disability prevention and the Indian NLEP context. Pair this with the dermatology common mistakes guide and the tuberculosis management deep dive for a complete mycobacterial map.
Mycobacterium leprae biology
- Acid-fast rod by Ziehl-Neelsen (modified Fite-Faraco for tissue sections, since standard ZN decolourises M. leprae).
- Obligate intracellular, lives mainly in Schwann cells of peripheral nerves and macrophages.
- Cannot be cultured in vitro — grown only in the mouse foot pad (Shepard, 1960) and the nine-banded armadillo (natural reservoir in the southern US).
- Generation time — 12 to 14 days; explains long incubation (2 to 10 years).
- Low temperature predilection — favours cooler body sites (skin, peripheral nerves, anterior eye, testes, upper respiratory mucosa); spares warm areas (axilla, groin, perineum, scalp).
- Transmission — predominantly droplet via nasal secretions of untreated LL/BL patients; entry via upper respiratory mucosa or broken skin. Household contacts at greatest risk.
- Genome — extensively decayed pseudogenes (about half the genome non-functional), explaining its dependence on host metabolism.
- Cell-mediated immunity dominates — strong CMI gives tuberculoid pole; weak CMI gives lepromatous pole.
Ridley-Jopling immunological spectrum
A 5-point spectrum based on CMI strength, lesion morphology, bacterial load, histology and lepromin response.
| Feature | TT | BT | BB | BL | LL |
|---|
| CMI | Strong | Strong-moderate | Unstable | Weak-moderate | Absent |
| Number of lesions | Single or few | Few | Several | Many | Numerous, symmetric |
| Lesion edge | Well-defined | Less well-defined | Punched-out (Swiss cheese) | Sloped | Diffuse |
| Anaesthesia | Marked | Moderate | Moderate | Mild | Late |
| Nerve thickening | One or few | Few | Several | Many | Many, symmetric |
| Bacilli on smear | Rare/absent | Few | Moderate | Many | Innumerable, globi |
| Lepromin | Strongly positive | Positive | Negative | Negative | Strongly negative |
| Histology | Epithelioid granuloma, no bacilli | Tuberculoid + nerves invaded | Mixed | Macrophages with foamy change | Foamy macrophages (Virchow cells) full of bacilli |
Indeterminate leprosy is the earliest, unclassified form — single hypopigmented patch, mild anaesthesia, often self-healing or progressing depending on host immunity.
Pure neuritic leprosy — nerve involvement without skin lesion; common in Indian patients.
Histoid leprosy — late LL with relapse after dapsone monotherapy; firm cutaneous nodules with spindle-cell histology.
WHO operational classification
For field implementation under NLEP, the WHO classifies by skin-lesion count and smear status:
- Paucibacillary (PB) — 1 to 5 skin lesions, negative slit-skin smear, mostly TT and BT, and single nerve trunk involvement.
- Multibacillary (MB) — more than 5 skin lesions, any positive slit-skin smear, or involvement of more than one nerve trunk. Includes BB, BL and LL.
The default in doubt is MB — undertreatment is the worse error.
Clinical features
Skin
- Hypopigmented, anaesthetic, anhidrotic patches (TT-BT).
- Numerous bilaterally symmetric copper-red infiltrated nodules and plaques (BL-LL).
- Leonine facies in LL — diffuse skin infiltration, thickened ears, loss of eyebrows (madarosis), saddle-nose deformity (nasal septum destruction).
Nerve involvement
Nerve trunks become palpably thickened — tested at predictable sites:
- Ulnar nerve — at the medial epicondyle; claw hand (ring and little fingers).
- Median nerve — at the wrist; ape thumb deformity, loss of opposition.
- Common peroneal nerve — at the fibular neck; foot drop.
- Posterior tibial nerve — at the medial malleolus; clawing of toes, plantar anaesthesia and trophic ulcers.
- Greater auricular nerve — visibly thickened in the neck.
- Facial nerve — zygomatic branch; lagophthalmos with corneal exposure.
- Radial cutaneous nerve — at the wrist; sensory loss.
Anaesthesia precedes motor loss in most cases — patients sustain burns and minor trauma without awareness, leading to acral injuries, secondary infection and shortening of digits.
Eye
Iritis (LL), lagophthalmos (CN VII palsy), corneal anaesthesia (CN V), secondary corneal ulceration, scleritis. Untreated leads to blindness.
Other sites
Testes (orchitis, atrophy, infertility, gynaecomastia in LL), nose (saddle-nose, anosmia, septal perforation), bone (resorption of phalanges), kidneys (amyloidosis in chronic LL).
Investigations
Slit-skin smear
Sample skin from six standard sites — both ear lobes, both eyebrows, chin, buttocks (and any active lesion). Slit the skin with a scalpel, scrape the dermis, smear on a slide, stain with modified Ziehl-Neelsen (Fite-Faraco), examine under oil immersion.
- Bacterial Index (BI) — Ridley logarithmic 0 to 6+ scale; counts acid-fast bacilli per oil-immersion field (0 = none; 6+ = greater than 1000 per field).
- Morphological Index (MI) — percent of bacilli that are solid-staining (live and uniformly stained); falls rapidly with treatment.
Skin biopsy
Confirms diagnosis and classifies along the spectrum. Look for granuloma type, nerve invasion, foamy (Virchow) macrophages and bacilli with Fite-Faraco.
Lepromin (Mitsuda) test
Intradermal injection of heat-killed M. leprae; read at 48 hours (Fernandez reaction, hypersensitivity) and 3 to 4 weeks (Mitsuda reaction, granulomatous). Positive in TT and BT; negative in LL. Not diagnostic — used for classification and prognosis. Useful for screening family contacts.
PCR
Increasingly used in research; not yet standard in NLEP field programmes.
WHO multidrug therapy (MDT) — 2018 update
To prevent rifampicin resistance, WHO 2018 standardised three-drug MDT for both PB and MB.
Adult regimens
Paucibacillary (6 months):
- Rifampicin 600 mg once monthly (supervised).
- Clofazimine 300 mg once monthly (supervised) plus 50 mg daily.
- Dapsone 100 mg daily.
Multibacillary (12 months):
- Same combination, duration extended to 12 months.
Drugs in brief
- Rifampicin — bactericidal; the single most important drug; kills 99.9 percent of viable bacilli within days. Side effects — hepatotoxicity, orange body fluids, flu-like syndrome.
- Clofazimine — bacteriostatic; anti-inflammatory action on ENL. Side effects — reddish-brown skin pigmentation (especially over lesions), ichthyosis, GI upset.
- Dapsone — bacteriostatic. Side effects — haemolysis (caution in G6PD deficiency), methaemoglobinaemia, agranulocytosis, dapsone hypersensitivity syndrome (DRESS), psychosis. Test for G6PD before starting in high-prevalence regions.
Pediatric and special doses
Weight-banded dosing for children. In pregnancy, MDT is safe and continued. Coinfection with HIV does not change MDT but raises reaction risk.
Post-MDT follow-up
Annual review for 2 years (PB) or 5 years (MB) to detect relapse and disability progression. Bacterial index should fall by 1 log per year.
Lepra reactions
Inflammatory exacerbations during or after MDT — not treatment failure. Continue MDT through reactions.
Type 1 (reversal) reaction
- Seen in — borderline leprosy (BT, BB, BL).
- Mechanism — delayed-type hypersensitivity (cell-mediated) flare; an upgrade or downgrade in CMI.
- Clinical — existing lesions become red, swollen and tender; acute neuritis with sudden nerve palsy and pain; oedema of hands and feet; no constitutional symptoms.
- Treatment — oral prednisolone 40 to 60 mg per day, tapered over 12 to 20 weeks. Continue MDT.
Type 2 (ENL — erythema nodosum leprosum) reaction
- Seen in — BL and LL.
- Mechanism — immune-complex (type III hypersensitivity); high circulating bacillary antigens trigger complement activation.
- Clinical — crops of tender, erythematous, subcutaneous nodules on extensor surfaces; fever, malaise; arthralgia, iritis, orchitis, lymphadenitis, glomerulonephritis. Multi-organ.
- Treatment — prednisolone (40 to 60 mg per day) for first episode; thalidomide 100 to 400 mg per day highly effective (males or women with strict contraception — fetal phocomelia is the classic teratogenic catastrophe); clofazimine in high dose (300 mg per day) for chronic ENL. Continue MDT.
Lucio phenomenon
Rare, severe vasculopathic reaction in untreated diffuse LL (Lucio leprosy), commonest in Mexican and Caribbean patients — angular necrotic ulcers, fever, vasculitis.
Disability and rehabilitation
WHO grades disability 0 to 2:
- Grade 0 — no disability.
- Grade 1 — anaesthesia of hand or foot or visual problems without visible deformity.
- Grade 2 — visible deformity (claw hand, foot drop, lagophthalmos, corneal opacity, plantar ulcer).
NLEP focuses on Grade 2 disability rate as the key indicator. Reconstructive surgery — tendon transfers for claw hand and foot drop, tarsorrhaphy for lagophthalmos, custom footwear for plantar ulcers.
NEET PG MCQ traps
- M. leprae cannot be cultured in vitro — only mouse foot pad and armadillo.
- Cool body parts preferentially involved; warm areas spared.
- Lepromin strongly positive in TT, negative in LL — measures CMI, not active infection.
- Slit-skin smear from six standard sites — both ear lobes, both eyebrows, chin, buttocks.
- Fite-Faraco stain for tissue sections (not standard ZN).
- PB = 1 to 5 lesions, smear negative; MB = greater than 5 lesions or smear positive.
- WHO MDT 2018 — three drugs (rifampicin + clofazimine + dapsone) for both PB and MB.
- Pure neuritic leprosy — common in India.
- Histoid leprosy — relapse after dapsone monotherapy.
- Type 1 reaction in borderline disease — steroids; thalidomide does NOT help.
- Type 2 (ENL) in BL/LL — thalidomide highly effective.
- Thalidomide teratogenicity — phocomelia; mandatory contraception.
- Dapsone + G6PD deficiency = haemolysis; check G6PD beforehand.
- Clofazimine — reddish-brown pigmentation; anti-inflammatory in ENL.
- Greater auricular nerve visibly thickened in the neck.
- Lagophthalmos — facial nerve zygomatic branch palsy; risk of corneal exposure.
- Saddle-nose, madarosis, leonine facies — late LL.
- BCG vaccination — provides partial protection against leprosy (60 to 80 percent against TT).
Recent updates and Indian context
- National Leprosy Eradication Programme (NLEP) — operational under National Health Mission since 1983. India achieved WHO elimination target (less than 1 per 10,000) at the national level in 2005, but several districts and states (Chhattisgarh, Odisha, Bihar, Dadra & Nagar Haveli) remain endemic with active transmission.
- India contributes about 60 percent of new global leprosy cases annually (over 100,000 cases per year per NLEP).
- Active Case Detection and Regular Surveillance for Leprosy (ACD&RS) and Leprosy Case Detection Campaigns (LCDC) — periodic door-to-door screening drives.
- Single-dose rifampicin (SDR) — given to all eligible household and neighbourhood contacts of newly diagnosed leprosy patients; introduced under NLEP in 2018 to interrupt transmission.
- WHO 2018 three-drug PB regimen — adopted by NLEP; clofazimine is no longer reserved for MB.
- Disability prevention and POD (Prevention of Disability) services — physiotherapy, protective footwear, self-care kits, reconstructive surgery — emphasised in the latest NLEP operational guidelines.
- Stigma reduction — Section 38 of the Rights of Persons with Disabilities Act 2016 includes leprosy-cured persons; the Personal Laws (Amendment) Act 2019 removed leprosy as a ground for divorce.
Frequently asked questions
What is the Ridley-Jopling classification?
The Ridley-Jopling classification places leprosy on a 5-point immunopathological spectrum based on cell-mediated immunity — tuberculoid (TT, strong CMI, few well-demarcated lesions, bacilli rare), borderline tuberculoid (BT), borderline borderline (BB, unstable), borderline lepromatous (BL) and lepromatous (LL, weak CMI, numerous lesions, abundant bacilli). Indeterminate leprosy is the earliest unclassified form. TT has a positive lepromin test and LL is lepromin-negative.
How does the WHO classify leprosy for treatment?
The WHO operational classification splits patients into paucibacillary (PB) — five or fewer skin lesions, negative slit-skin smear, mostly tuberculoid and borderline tuberculoid — and multibacillary (MB) — more than five skin lesions, any positive smear, or involvement of more than one nerve trunk; includes BB, BL and LL. PB receives a 6-month MDT regimen (rifampicin, dapsone, clofazimine in WHO 2018 update); MB receives 12 months.
What is the WHO multidrug therapy (MDT) regimen?
The 2018 WHO update standardised three-drug MDT for both PB and MB to prevent rifampicin resistance. PB receives 6 months — rifampicin 600 mg once monthly supervised, clofazimine 300 mg monthly supervised plus 50 mg daily, and dapsone 100 mg daily. MB receives the same combination for 12 months. Children and underweight adults receive weight-based doses. Free supply through NLEP across India.
What is the lepromin (Mitsuda) test?
The lepromin test injects heat-killed Mycobacterium leprae intradermally and reads the response at 48 hours (Fernandez reaction — early hypersensitivity) and 3 to 4 weeks (Mitsuda reaction — granulomatous reaction). It assesses cell-mediated immunity, not active infection. It is strongly positive in tuberculoid leprosy (TT) and unaffected family contacts, and negative in lepromatous leprosy (LL). It is not used for diagnosis but for classification and prognosis.
How do type 1 and type 2 lepra reactions differ?
Type 1 (reversal) reaction is a delayed-type hypersensitivity flare seen in borderline leprosy (BT, BB, BL) — existing skin lesions become red, swollen and tender, and acute neuritis can cause sudden nerve palsy. Treat with oral prednisolone 40 to 60 mg per day tapered over 12 to 20 weeks. Type 2 reaction (erythema nodosum leprosum, ENL) is an immune-complex reaction seen in BL and LL — crops of tender erythematous nodules, fever, arthralgia, iritis, orchitis. Treat with prednisolone, thalidomide (males or strict contraception) or clofazimine.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026