Version 1.0 — Published April 2026
Quick Answer
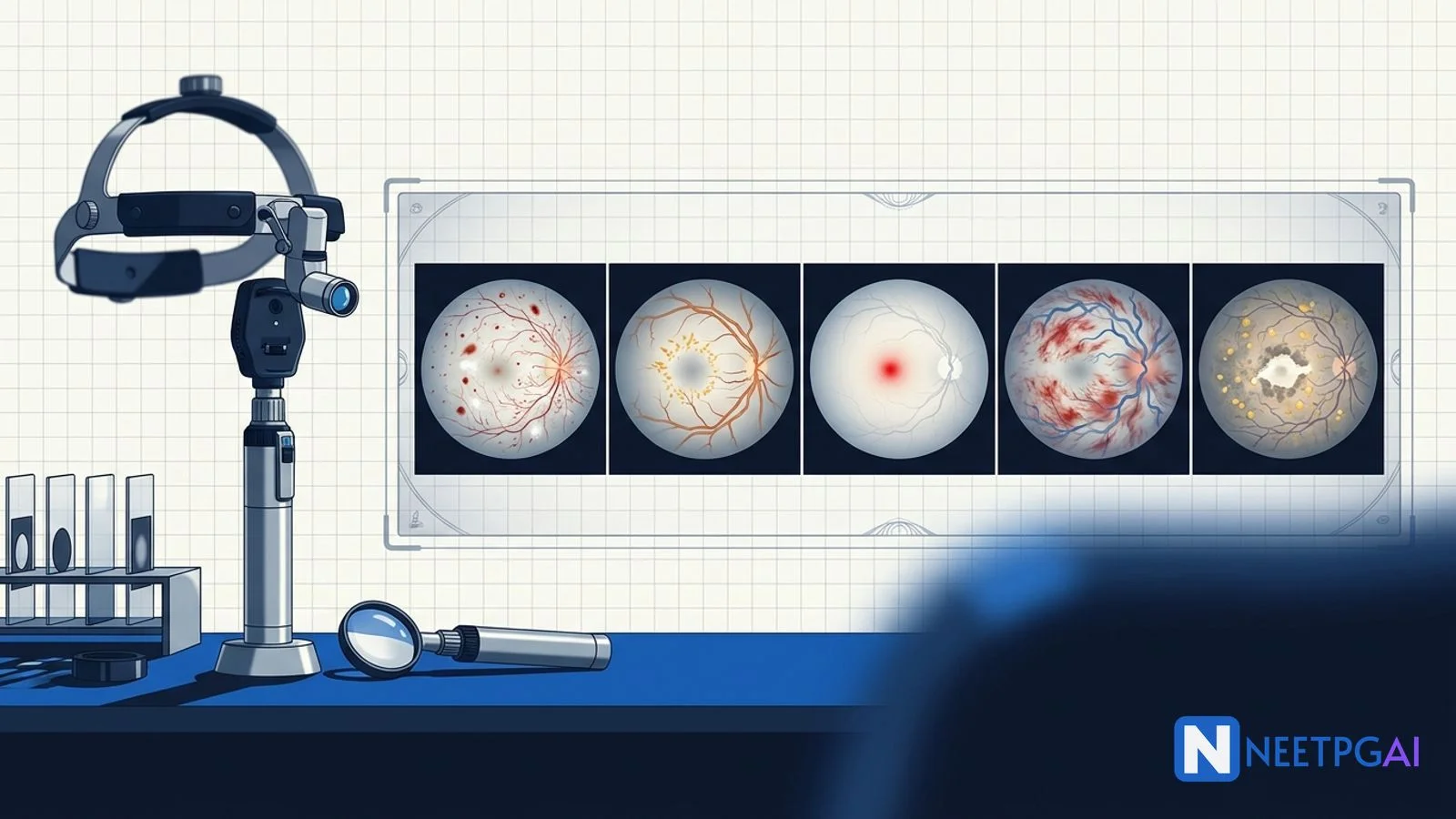
Fundoscopy image MCQs contribute 4-5 questions per NEET PG paper across ophthalmology, medicine, and endocrinology. Five retinal patterns recur reliably: diabetic retinopathy (microaneurysms, dot-blot hemorrhages, cotton-wool spots, neovascularization), hypertensive retinopathy (AV nicking, copper/silver wiring, papilledema in Grade 4), CRAO (cherry-red spot on pale retina), CRVO (blood-and-thunder fundus), and age-related macular degeneration (drusen, geographic atrophy, choroidal neovascularization).
The pattern-to-diagnosis mapping plus the high-yield management algorithm (laser, anti-VEGF, BP control, embolic workup) covers nearly every retinal NEET PG question across recent papers.
Why fundoscopy image MCQs are high-yield
Indian medical curricula keep fundoscopy in the practical exam, and NEET PG examiners follow with a steady 4-5 retinal images per paper. Diabetic retinopathy alone yields 2-3 questions (often paired with a Type 2 DM vignette), and hypertensive retinopathy is staple material in the medicine and PSM sections. CRAO and CRVO are emergency-medicine MCQs that reward rapid pattern recognition and the right time-window answer. AMD increasingly appears as a geriatrics or AI-Overview question and tests the dry-vs-wet distinction.
For each MCQ below, we walk through the image description, four answer options, the correct answer with reasoning, and a teaching pearl. Drill these five patterns plus 10 daily fundus images for 2 weeks and your accuracy will move from 35 to 80 percent.
MCQ 1: 52-year-old man with type 2 diabetes for 14 years and recent vision change
Image description: [Colour fundus photograph of the right eye showing the optic disc and macula. Multiple small round red dots (microaneurysms) are scattered in the macular region. Several blot hemorrhages are visible in the deep retinal layers, especially in the supero-temporal arcade. Two cotton-wool spots (fluffy white lesions) are seen along the inferior arcade. New tufts of fine, lacy vessels are growing on the optic disc surface (NVD) and at the supero-temporal arcade (NVE). A few hard exudates form a partial circinate ring near the fovea. The arcade veins show mild beading. No vitreous hemorrhage.]
Clinical vignette: A 52-year-old businessman with poorly controlled Type 2 diabetes (HbA1c 9.6 percent) for 14 years presents with painless gradual blurring of vision in his right eye for 6 weeks. He has hypertension and dyslipidemia. Visual acuity is 6/24 right, 6/12 left. IOP is normal in both eyes.
Options:
- (a) Moderate non-proliferative diabetic retinopathy with clinically significant macular oedema
- (b) Proliferative diabetic retinopathy
- (c) Hypertensive retinopathy Grade 3
- (d) Branch retinal vein occlusion
Correct answer: (b) Proliferative diabetic retinopathy
Reasoning: The presence of neovascularization at the disc (NVD) and neovascularization elsewhere (NVE) defines proliferative diabetic retinopathy, regardless of how many other NPDR features (microaneurysms, dot-blot hemorrhages, cotton-wool spots, hard exudates, venous beading) are also present. PDR is the threshold for pan-retinal photocoagulation (PRP) plus intravitreal anti-VEGF therapy.
Moderate NPDR shows microaneurysms, hemorrhages, hard exudates without the 4-2-1 severe NPDR criteria, and crucially without neovascularization. Hypertensive Grade 3 retinopathy would emphasise AV nicking, copper wiring, and a macular star of hard exudates without microaneurysms. BRVO produces sectoral hemorrhages confined to the territory of one retinal vein, not the diffuse mid-peripheral pattern of diabetic retinopathy.
Teaching pearl: ETDRS / international classification of diabetic retinopathy:
| Stage | Findings |
|---|
| No DR | No abnormalities |
| Mild NPDR | Microaneurysms only |
| Moderate NPDR | More than just microaneurysms but less than severe |
| Severe NPDR | 4-2-1 rule: severe hemorrhages in 4 quadrants, OR venous beading in 2 quadrants, OR IRMA in 1 quadrant |
| PDR | Neovascularization (NVD or NVE) and/or vitreous/preretinal hemorrhage |
Diabetic macular oedema (DMO) is a separate axis that can coexist with any DR stage. Clinically significant macular oedema (CSMO — old ETDRS criteria) is now largely replaced by OCT-based measurement of central macular thickness. Anti-VEGF (ranibizumab, aflibercept, bevacizumab) is the first-line therapy for centre-involving DMO.
Management of PDR:
- Pan-retinal photocoagulation (PRP) — gold-standard ablation of ischemic peripheral retina; reduces VEGF drive and induces regression of new vessels
- Intravitreal anti-VEGF — alternative or adjunct; useful in vitreous hemorrhage limiting laser delivery
- Vitrectomy — for non-clearing vitreous hemorrhage, traction retinal detachment, combined traction-rhegmatogenous detachment
Risk reduction targets: HbA1c <7 percent (DCCT/UKPDS), BP <130/80, statin therapy, and annual screening fundoscopy from diagnosis in T2DM and from 5 years post-diagnosis in T1DM (or as guided by ICMR / All-India guidelines for India).
MCQ 2: 48-year-old man with severe headache and BP 220/130 mmHg
Image description: [Colour fundus photograph of the right eye showing a swollen, blurred optic disc with elevated margins (papilledema). Surrounding the disc are flame-shaped hemorrhages and several cotton-wool spots. The macular region shows a partial star-shaped pattern of hard yellow exudates radiating from the fovea (macular star). The retinal arterioles are markedly narrowed, with focal constrictions at AV crossings (Salus sign — AV nicking) and a diffuse copper-coloured light reflex. One arteriole shows a more silvery sheen distally.]
Clinical vignette: A 48-year-old taxi driver presents with a 3-day history of severe occipital headache, blurring of vision, and one episode of vomiting. BP is 220/130 mmHg in both arms. Urine dipstick shows trace proteinuria. Creatinine is 1.6 mg/dL.
Options:
- (a) Hypertensive retinopathy Grade 2 (KWB)
- (b) Hypertensive retinopathy Grade 4 (KWB) — malignant hypertension
- (c) Diabetic retinopathy with macular oedema
- (d) Idiopathic intracranial hypertension
Correct answer: (b) Hypertensive retinopathy Grade 4 (KWB) — malignant hypertension
Reasoning: Papilledema is the defining feature of KWB Grade 4 hypertensive retinopathy and signifies malignant (accelerated) hypertension — a hypertensive emergency. The presence of flame hemorrhages, cotton-wool spots, hard exudates with macular star, AV nicking, and copper/silver wiring on a background of dramatically elevated BP confirms the diagnosis.
KWB Grade 2 has AV nicking and copper wiring but no hemorrhages, exudates, or papilledema. Diabetic retinopathy features microaneurysms and dot-blot hemorrhages (deep retinal); hypertensive retinopathy features flame hemorrhages (nerve fibre layer) — the morphology helps differentiate when both are listed. Idiopathic intracranial hypertension shows papilledema but without retinal hemorrhages, exudates, AV nicking, or systemic hypertensive findings.
Teaching pearl: Keith-Wagener-Barker classification:
| Grade | Findings |
|---|
| Grade 1 | Mild generalised arteriolar narrowing, increased light reflex (copper wiring) |
| Grade 2 | Focal arteriolar narrowing, AV nicking (Salus sign), more pronounced sclerosis (silver wiring), Gunn sign (vein deviated at AV crossing), Bonnet sign (banking proximal to crossing) |
| Grade 3 | Grade 2 plus flame hemorrhages, cotton-wool spots, hard exudates (macular star) |
| Grade 4 | Grade 3 plus papilledema — malignant or accelerated hypertension |
Pathophysiology pearls:
- Copper wiring — moderate arteriolar wall thickening reflects light with a coppery sheen
- Silver wiring — severe sclerosis, vessel appears as a silver thread; the column of blood is no longer visible
- AV nicking (Salus sign) — the thickened arteriolar wall compresses the underlying vein at crossings
- Cotton-wool spots — retinal nerve-fibre layer infarcts from arteriolar occlusion
- Macular star — exudates radiate along Henle fibre layer of the macula
Management of malignant hypertension (KWB Grade 4 + neurologic, cardiac, or renal end-organ damage): IV labetalol, nicardipine, or nitroprusside; lower MAP by no more than 20-25 percent in the first 1-2 hours (precipitous falls cause watershed strokes), then to 160/100 over 6 hours, then to normal over 24-48 hours. Investigate for secondary causes (renal artery stenosis, pheochromocytoma, primary aldosteronism, coarctation, OSA).
MCQ 3: 68-year-old woman with sudden painless monocular vision loss
Image description: [Colour fundus photograph of the left eye showing a diffusely pale, milky-white retinal background with attenuated, narrow retinal arterioles. The optic disc is mildly pale. At the centre of the macula there is a strikingly bright red oval spot (cherry-red spot) sharply contrasting against the pale surrounding retina. No retinal hemorrhages, no neovascularization, no exudates. A faint cilio-retinal artery near the disc supplies a small island of normally perfused retina just temporal to the disc.]
Clinical vignette: A 68-year-old woman with hypertension, atrial fibrillation (off anticoagulation), and prior left carotid endarterectomy presents to the emergency department with sudden painless complete loss of vision in her left eye 2 hours ago. Visual acuity is light perception only in the affected eye. Pupil shows a relative afferent pupillary defect.
Options:
- (a) Central retinal vein occlusion
- (b) Central retinal artery occlusion
- (c) Vitreous hemorrhage
- (d) Optic neuritis
Correct answer: (b) Central retinal artery occlusion (CRAO)
Reasoning: Cherry-red spot on a pale retina with attenuated arterioles, in a patient with embolic risk factors (AF, prior carotid surgery), and sudden painless monocular vision loss is the canonical presentation of central retinal artery occlusion. The cherry-red spot reflects intact choroidal blood supply visible through the thin foveal floor, against a milky-white infarcted surrounding retina with full-thickness inner-retinal swelling.
CRVO produces blood-and-thunder fundus with diffuse hemorrhages, dilated tortuous veins, and disc swelling — not a pale retina with cherry-red spot. Vitreous hemorrhage obscures the fundus view altogether; you cannot see the optic disc clearly. Optic neuritis presents with painful vision loss (eye movement worsens pain), normal disc in retrobulbar neuritis, or mild disc swelling in papillitis — without the cherry-red spot.
Teaching pearl: Cherry-red spot — the high-yield NEET PG association list:
| Disease | Pathomechanism |
|---|
| Central retinal artery occlusion | Inner retinal infarction; choroid visible through fovea |
| Tay-Sachs disease (GM2 gangliosidosis) | Lysosomal storage; ganglion cells filled with gangliosides |
| Niemann-Pick disease type A and B | Sphingomyelinase deficiency; sphingomyelin accumulation |
| Sandhoff disease | Hexosaminidase A and B deficiency |
| GM1 gangliosidosis | β-galactosidase deficiency |
| Sialidosis (cherry-red spot myoclonus syndrome) | Sialidase deficiency |
| Krabbe disease (less commonly) | Galactocerebrosidase deficiency |
| Quinine, methanol, dapsone toxicity | Drug-induced retinal damage |
| Commotio retinae (Berlin oedema) | Blunt trauma; transient |
Management of CRAO — the time window is <90 minutes for high recovery, 90-240 minutes for variable recovery, beyond which retinal infarction is generally permanent:
- Ocular massage — to dislodge embolus distally
- Lower IOP — IV acetazolamide 500 mg, topical timolol, anterior chamber paracentesis
- Carbogen / inhalation 5 percent CO2 in 95 percent O2 — induces retinal vasodilatation
- Sublingual nitrate — questionable efficacy
- Intra-arterial fibrinolysis (rare, specialised centres) — emerging; not standard
- Investigate for embolic source — carotid Doppler, echocardiogram, holter, fasting lipids, FBS, ESR/CRP (rule out giant cell arteritis if >50; high-dose steroids if positive)
- Long-term secondary prevention — antiplatelet, statin, BP and DM control, anticoagulation if cardioembolic source
Always rule out giant cell arteritis (GCA) in patients ≥50 with CRAO — temporal artery tenderness, jaw claudication, headache, polymyalgic symptoms, raised ESR/CRP. Empirical high-dose IV methylprednisolone before temporal artery biopsy can save the contralateral eye.
MCQ 4: 60-year-old man with sudden blurring of vision and known hypertension
Image description: [Colour fundus photograph of the right eye showing massive scattered retinal hemorrhages in all four quadrants — flame-shaped hemorrhages in the nerve fibre layer and dot-and-blot hemorrhages in the deeper retinal layers. The retinal veins are markedly dilated, tortuous, and engorged. The optic disc is hyperaemic and swollen, with blurred margins. Multiple cotton-wool spots are present along all the vascular arcades. Macular oedema is evident as a thickened greyish appearance of the central retina. The retinal arteries appear relatively normal in caliber.]
Clinical vignette: A 60-year-old man with long-standing hypertension and Type 2 diabetes presents with sudden painless blurring of vision in his right eye 3 days ago. Visual acuity is 6/60 right, 6/9 left. IOP is 18 mmHg right, 14 mmHg left.
Options:
- (a) Central retinal artery occlusion
- (b) Central retinal vein occlusion (blood-and-thunder fundus)
- (c) Proliferative diabetic retinopathy with vitreous hemorrhage
- (d) Hypertensive retinopathy Grade 3
Correct answer: (b) Central retinal vein occlusion (blood-and-thunder fundus)
Reasoning: Diffuse hemorrhages in all four quadrants plus dilated tortuous veins plus disc swelling is the textbook blood-and-thunder fundus of CRVO. Hypertension and diabetes are the two most common risk factors. The painless onset, preserved arterial caliber, and dramatic venous engorgement distinguish CRVO from CRAO and other diagnoses.
CRAO would show pale retina with cherry-red spot and arteriolar attenuation — not hemorrhages. PDR with vitreous hemorrhage typically shows neovascularization and the hemorrhage often obscures retinal detail; even when retinal detail is visible, hemorrhages tend to be peripheral and less diffuse. Hypertensive retinopathy Grade 3 has flame hemorrhages and cotton-wool spots but with copper wiring, AV nicking, and normal venous caliber — not the dilated tortuous veins of CRVO.
Teaching pearl: CRVO classification and complications:
| Type | Features | Risk |
|---|
| Non-ischemic CRVO | Less than 10 disc-areas of capillary non-perfusion on FFA, mild RAPD, better visual prognosis | Lower risk of neovascular glaucoma |
| Ischemic CRVO | More than 10 disc-areas of capillary non-perfusion, dense RAPD, worse vision | High risk of "90-day glaucoma" — neovascular glaucoma at 3 months from iris and angle neovascularization |
Management of CRVO:
- Anti-VEGF intravitreal injections (ranibizumab, aflibercept, bevacizumab) — first-line for macular oedema causing visual impairment; monthly initially, then PRN
- Intravitreal dexamethasone implant (Ozurdex) — alternative for steroid-responsive patients or those needing less frequent injections
- Pan-retinal photocoagulation (PRP) — for ischemic CRVO with neovascularization (iris, angle, or retina) to prevent / treat neovascular glaucoma
- Treat systemic risk factors — hypertension, diabetes, hyperlipidaemia, glaucoma; rule out hyperviscosity syndromes (myeloma, polycythemia), thrombophilia in young patients
- Anticoagulation is NOT routinely indicated — CRVO is generally not embolic; aspirin not consistently beneficial
BRVO (branch retinal vein occlusion) is a unilateral sectoral version — hemorrhages confined to the territory of one retinal vein (most commonly supero-temporal). Treated similarly with anti-VEGF, sectoral laser, and risk-factor control.
MCQ 5: 78-year-old woman with gradual central vision distortion
Image description: [Colour fundus photograph of the macula of the left eye showing multiple yellow-white round deposits of varying sizes (drusen) clustered around the fovea — both small hard drusen (less than 63 micrometres, sharply defined) and larger soft drusen (over 125 micrometres, indistinct margins). Pigmentary changes (focal hyperpigmentation and depigmentation) are seen at the RPE level. A sharply demarcated area of RPE and outer-retinal atrophy is visible just inferior to the fovea, with underlying choroidal vessels clearly visible through the atrophic patch (geographic atrophy). No subretinal hemorrhage, no fluid, no neovascular membrane.]
Clinical vignette: A 78-year-old retired teacher presents with 6 months of gradually worsening central vision in both eyes — she struggles to read newsprint and finds straight lines slightly distorted on the Amsler grid. She is a former smoker, has mild hypertension, and has a strong family history of "central blindness." Visual acuity is 6/24 left, 6/18 right. IOP and anterior segment are normal bilaterally.
Options:
- (a) Diabetic macular oedema
- (b) Wet (neovascular) age-related macular degeneration
- (c) Dry (non-exudative) age-related macular degeneration with geographic atrophy
- (d) Central serous chorioretinopathy
Correct answer: (c) Dry (non-exudative) age-related macular degeneration with geographic atrophy
Reasoning: Drusen plus pigmentary changes plus a sharply demarcated area of RPE and outer-retinal atrophy without subretinal hemorrhage or fluid is dry AMD with geographic atrophy — the most advanced form of non-exudative AMD. Age >75, smoking history, and family history are classic risk factors.
Wet AMD would show subretinal hemorrhage, lipid exudates, sub-RPE or subretinal fluid, and a choroidal neovascular membrane (CNV) — none present here. Diabetic macular oedema would show microaneurysms, dot-blot hemorrhages, and hard exudates with diabetic background; no drusen. Central serous chorioretinopathy presents in middle-aged males (Type A personality, steroid use) with a serous retinal detachment at the macula and a smokestack on FFA — not drusen and atrophy.
Teaching pearl: AMD categorisation (AREDS / Beckman / international):
| Category | Features |
|---|
| No AMD | No drusen or only small (drupelet) drusen ≤63 micrometres |
| Early AMD | Medium drusen (63-125 micrometres), no pigmentary changes |
| Intermediate AMD | Large drusen (>125 micrometres) and/or pigmentary changes |
| Late AMD: dry (geographic atrophy) | RPE and outer retinal atrophy ≥250 micrometres in greatest dimension |
| Late AMD: wet (neovascular) | Choroidal neovascular membrane (Type 1 sub-RPE, Type 2 subretinal, Type 3 RAP, polypoidal choroidal vasculopathy) |
Management:
- Dry AMD intermediate — AREDS2 vitamins (vitamin C 500 mg, vitamin E 400 IU, lutein 10 mg, zeaxanthin 2 mg, zinc 80 mg, copper 2 mg) — reduce 5-year progression to advanced AMD by ~25 percent. Beta-carotene removed from AREDS2 due to lung cancer risk in smokers
- Dry AMD with geographic atrophy — pegcetacoplan (C3 inhibitor) and avacincaptad pegol (C5 inhibitor) recently FDA-approved to slow progression of GA; not yet widely available in India
- Wet AMD — intravitreal anti-VEGF (ranibizumab, aflibercept, bevacizumab off-label, brolucizumab, faricimab) is the standard of care; monthly induction then PRN or treat-and-extend regimens
- Lifestyle — smoking cessation (single most important modifiable risk factor), Mediterranean / leafy-green diet, UV protection
- Low-vision rehabilitation — magnifiers, eccentric viewing training; preserves quality of life
Amsler grid self-monitoring is the high-yield home tool — patients with intermediate AMD should check daily and report new metamorphopsia immediately for prompt OCT and anti-VEGF if wet conversion is detected.
Common pitfalls — patterns that can be confused
Pitfall 1: Diabetic retinopathy versus hypertensive retinopathy
Both can show hemorrhages and exudates. Diabetic retinopathy features microaneurysms and dot-and-blot deep hemorrhages with hard exudates and neovascularization; hypertensive retinopathy features flame-shaped superficial hemorrhages with copper/silver wiring, AV nicking, and macular star pattern of exudates. Cotton-wool spots can appear in both. Coexisting diabetes and hypertension produce a mixed picture — comment on both etiologies.
Pitfall 2: CRAO versus CRVO
CRAO = pale retina, cherry-red spot, attenuated arterioles, sudden complete vision loss within minutes, RAPD strongly positive. CRVO = blood-and-thunder fundus with hemorrhages, dilated tortuous veins, swollen disc, subacute partial vision loss over hours to days. Both have RAPD, but CRAO is denser. CRAO is an emergency with a 90-240 minute reperfusion window; CRVO is treated electively with anti-VEGF.
Pitfall 3: AMD versus diabetic macular oedema versus CSCR
Macular pathology in an elderly patient with drusen and atrophy — AMD. Macular pathology in a diabetic with microaneurysms and hemorrhages — DMO. Macular pathology in a young/middle-aged man with serous detachment, recent steroid use or stress — CSCR. OCT and FFA confirm.
Pitfall 4: Cherry-red spot in CRAO versus storage diseases
In CRAO the cherry-red spot is acquired (hours to days), unilateral, with arteriolar attenuation and history of vascular risk factors. In gangliosidoses (Tay-Sachs, Niemann-Pick) it is bilateral, develops in infancy, and accompanies developmental regression and hepatosplenomegaly — a paediatric vignette.
Pitfall 5: Papilledema versus pseudopapilledema versus optic neuritis
Papilledema (KWB Grade 4 hypertension, raised ICP) shows bilateral disc swelling with elevated margins, loss of physiological cup, peripapillary hemorrhages, and Paton lines; vision usually preserved early. Pseudopapilledema (optic disc drusen) is congenital, no peripapillary hemorrhages, autofluorescent on B-scan ultrasound. Optic neuritis is unilateral, painful with eye movement, RAPD, and central scotoma.
Frequently Asked Questions
How do you differentiate non-proliferative from proliferative diabetic retinopathy on fundoscopy?
Non-proliferative diabetic retinopathy (NPDR) shows microaneurysms, dot-and-blot hemorrhages, hard exudates, cotton-wool spots, venous beading, and intraretinal microvascular abnormalities (IRMA) — but no neovascularization. Severe NPDR is defined by the 4-2-1 rule (severe hemorrhages in 4 quadrants, OR venous beading in 2 quadrants, OR IRMA in 1 quadrant). Proliferative diabetic retinopathy (PDR) requires neovascularization at the disc (NVD) or elsewhere in the retina (NVE), and may be complicated by vitreous hemorrhage, traction retinal detachment, or neovascular glaucoma. PDR is treated with pan-retinal photocoagulation, intravitreal anti-VEGF injections, or vitrectomy.
What is the Keith-Wagener-Barker classification of hypertensive retinopathy?
Keith-Wagener-Barker (KWB) classification grades hypertensive retinopathy: Grade 1 — mild generalised arteriolar narrowing or sclerosis, increased light reflex (copper wiring); Grade 2 — definite arteriolar narrowing with focal areas of constriction, AV nicking (Salus sign), more pronounced sclerosis (silver wiring); Grade 3 — Grade 2 plus retinal hemorrhages, hard exudates (often macular star), and cotton-wool spots; Grade 4 — Grade 3 plus papilledema (optic disc swelling), defining malignant or accelerated hypertension. KWB Grade 4 is a hypertensive emergency requiring urgent BP lowering with IV labetalol or nicardipine to a safe target while avoiding precipitous falls.
What causes the cherry-red spot in central retinal artery occlusion?
In central retinal artery occlusion (CRAO), the retina infarcts and becomes pale and oedematous from ischemic intracellular swelling. The fovea has no inner retinal layers — only the choroidal blood supply visible through the thin foveal floor. While the surrounding ischemic retina turns milky white, the fovea retains its normal red colour from the underlying choroid, producing the characteristic 'cherry-red spot' against a pale background. CRAO is an ophthalmic emergency: vision recovery requires reperfusion within 90 to 240 minutes — beyond this window, retinal infarction is permanent. Investigate for embolic source (carotid Doppler, echo, ESR for giant cell arteritis if over 50).
What does the blood-and-thunder fundus appearance signify?
Blood-and-thunder fundus is the classic appearance of central retinal vein occlusion (CRVO). Features include diffuse retinal hemorrhages in all four quadrants (often flame-shaped in the nerve fibre layer and dot-blot in deeper layers), dilated tortuous retinal veins, optic disc swelling, cotton-wool spots, and macular oedema. CRVO is sub-classified into non-ischemic (better prognosis, less neovascularization risk) and ischemic (extensive capillary non-perfusion on FFA, high risk of neovascular glaucoma — the dreaded '90-day glaucoma'). Treatment is intravitreal anti-VEGF (ranibizumab, aflibercept) for macular oedema; pan-retinal photocoagulation for ischemic CRVO with neovascularization.
How do dry and wet age-related macular degeneration differ on fundoscopy?
Dry (non-exudative) AMD, accounting for 85 to 90 percent of cases, shows drusen (small yellow-white deposits beneath the retinal pigment epithelium), pigmentary changes, and in advanced disease geographic atrophy — sharply demarcated areas of RPE and outer-retinal loss. Vision loss is gradual and central. Wet (neovascular, exudative) AMD shows choroidal neovascular membrane (CNV) breaking through Bruch's membrane, producing subretinal hemorrhage, lipid exudates, sub-RPE fluid, and rapid central vision loss often associated with metamorphopsia (distorted vision on Amsler grid). Wet AMD is treated with intravitreal anti-VEGF; dry AMD has no proven pharmacological therapy except AREDS2 vitamins for intermediate disease to reduce progression.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: April 2026