Version 1.0 — Published May 2026
Quick Answer
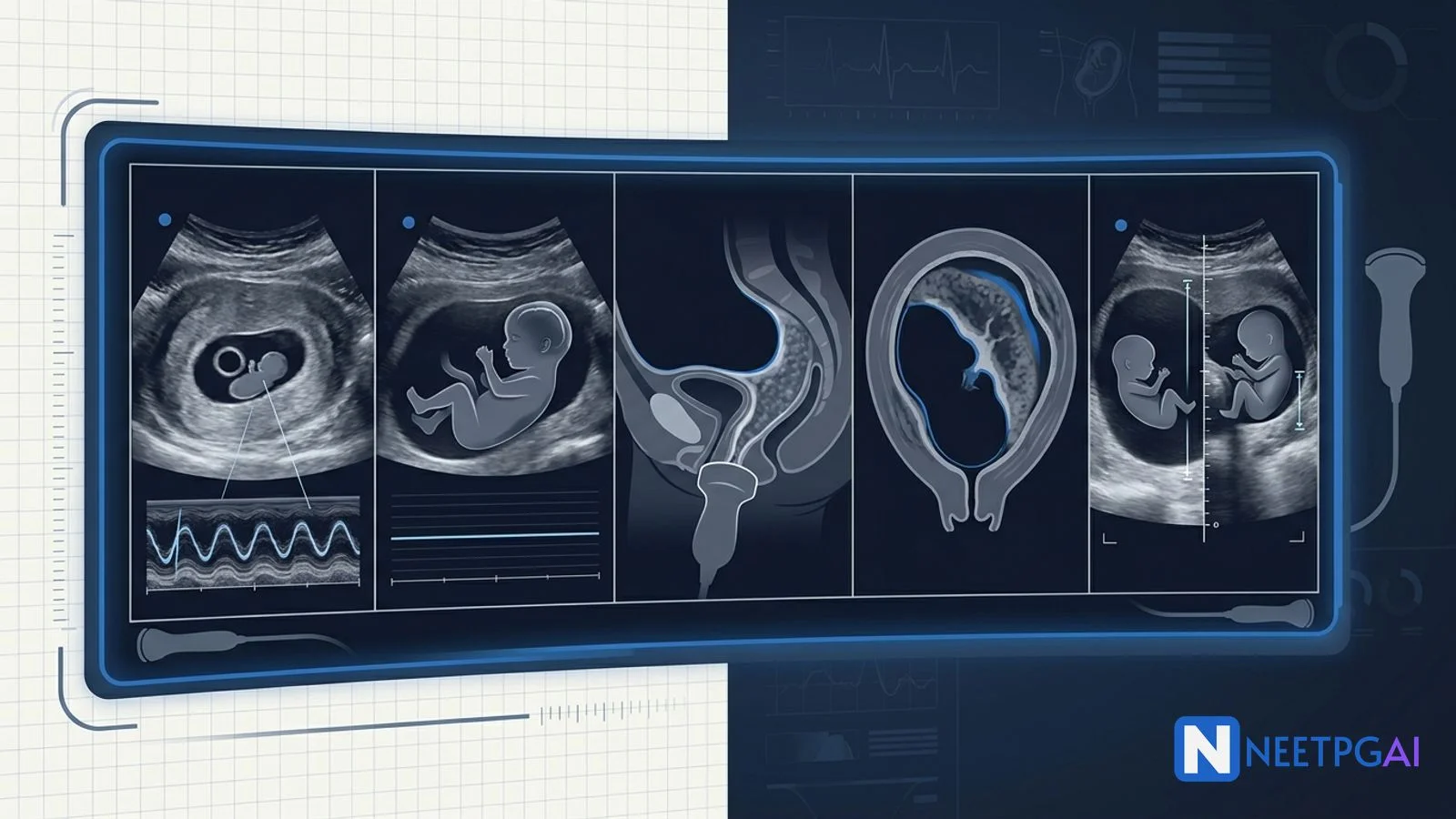
Obstetric ultrasound contributes 4-6 image-based MCQs per NEET PG paper, primarily under OBG and radiology. Five high-yield patterns recur reliably across years:
- Early pregnancy assessment — gestational sac with yolk sac and double-decidual sign by 5-6 weeks; anembryonic gestation if MSD over 25 mm with no embryo
- Intrauterine fetal demise (IUFD) — absent cardiac activity at CRL of 7 mm or more; late Spalding, Robert, and Deuel signs
- Placenta previa — placenta covering the internal os on TVS; modern RCOG 2018 simplified two-category classification (previa vs low-lying)
- Placental abruption — retroplacental hematoma; concealed (20 percent, higher fetal mortality) vs revealed (80 percent); clinical more than sonographic diagnosis
- Amniotic fluid abnormalities — polyhydramnios (AFI over 25 cm or DVP over 8 cm) vs oligohydramnios (AFI under 5 cm or DVP under 2 cm), and their causes
Combining gestational age, sonographic findings, and maternal clinical context collapses almost every obstetric USG MCQ into a 30-60 second answer.
Why obstetric USG image MCQs are high-yield for NEET PG
Obstetric ultrasound is the workhorse investigation of pregnancy in India — at every level of care from PHCs (handheld portable USG under the LaQshya programme) to tertiary centres. The diagnostic patterns are stereotyped and reproducible, making them ideal for image-based MCQs. NEET PG, INI-CET, and FMGE feature obstetric USG images in 4-6 questions per paper, often coupled with a clinical vignette to test pattern recognition, gestational-age awareness, and management decisions.
Drilling these 5 patterns plus 10-15 additional PYQ images (twin pregnancy types, fetal anomalies, hydrops, ectopic pregnancy, molar pregnancy, cervical insufficiency) over 2-3 weeks moves accuracy from 40 to 80 percent in this domain.
Foundational approach before the MCQs
Systematic obstetric USG read
| Step | What to look at | Common abnormalities |
|---|
| Uterus | Size, contour, fundal height, scars | Lower segment, contraction ring, fibroids, anomalies |
| Gestational sac | Location, MSD, eccentric implantation, double-decidual sign | Ectopic, anembryonic, subchorionic hematoma |
| Yolk sac and embryo | Yolk sac presence, CRL, cardiac activity | IUFD, anembryonic, blighted ovum |
| Placenta | Location (anterior/posterior/fundal/low), relation to internal os, thickness, lakes | Previa, abruption, accreta, succenturiate lobe |
| Cervix | Length on TVS, internal os, funneling | Cervical insufficiency (under 25 mm before 24 weeks) |
| Amniotic fluid | AFI or DVP | Polyhydramnios, oligohydramnios, anhydramnios |
| Fetus | Anatomy survey, growth (BPD, HC, AC, FL), Doppler | Anomalies, IUGR, macrosomia |
| Adnexa | Corpus luteum, ovarian cysts, masses | Ectopic, hyperstimulation, torsion |
Gestational-age-based mental shortlists
| Gestation | Expected USG finding | Common pathologies |
|---|
| 4-6 weeks | Gestational sac, yolk sac, fetal pole | Anembryonic, missed miscarriage, ectopic |
| 6-12 weeks | CRL measurement, cardiac activity, NT | IUFD, threatened abortion, molar pregnancy |
| 18-21 weeks | Anomaly scan; placental location; AFI | Anomalies, low-lying placenta |
| 24-28 weeks | Growth, biophysical profile, cervix | IUGR, gestational diabetes effects |
| 32-36 weeks | Repeat placenta location, growth | Previa migration, IUGR, malpresentation |
| Term (37+ weeks) | Growth, AFI, BPP, Doppler | Macrosomia, IUGR, oligohydramnios, post-term changes |
MCQ 1: 27-year-old woman with 6 weeks amenorrhea on early ultrasound
Image description: [Transvaginal ultrasound (TVS) of the uterus in a 27-year-old G1 woman with 6 weeks amenorrhea by LMP and a positive urine pregnancy test. Image shows an eccentrically implanted gestational sac in the fundal endometrium measuring approximately 18 mm in mean sac diameter (MSD). Inside the sac is a clearly visible yolk sac (a circular anechoic structure with bright echogenic rim, 4 mm diameter). Adjacent to the yolk sac is a small embryonic pole, approximately 4 mm CRL, with visible cardiac activity on M-mode of approximately 110 beats per minute. Surrounding the gestational sac, the double-decidual sign is visible — two concentric echogenic rings (decidua parietalis and decidua capsularis) with a thin anechoic line between them. The endometrium elsewhere is thickened (15 mm). No subchorionic hematoma. Both ovaries normal with a corpus luteum cyst on the right.]
Clinical vignette: A 27-year-old primigravida presents to the OBG outpatient department with 6 weeks amenorrhea and a positive urine pregnancy test confirmed at home 2 weeks earlier. She is asymptomatic — no vaginal bleeding, no abdominal pain, mild nausea in the mornings. She is anxious as her sister had an ectopic pregnancy last year. Beta-hCG is 8500 mIU/mL. Transvaginal ultrasound is performed.
Options:
- (a) Normal early intrauterine pregnancy of approximately 6 weeks
- (b) Anembryonic gestation (blighted ovum)
- (c) Ectopic pregnancy with pseudosac
- (d) Subchorionic hematoma with threatened abortion
Correct answer: (a) Normal early intrauterine pregnancy of approximately 6 weeks
Reasoning: Eccentric implantation of a gestational sac with double-decidual sign, visible yolk sac, and a 4 mm embryo with cardiac activity is textbook normal early intrauterine pregnancy at 6 weeks. The combination of double-decidual sign + yolk sac is highly specific for intrauterine pregnancy and excludes pseudosac (centrally placed fluid collection seen in ectopic, no yolk sac, single decidual ring). Beta-hCG of 8500 mIU/mL is consistent with 6 weeks (discriminatory zone for TVS visualisation of intrauterine pregnancy is 1500-2000 mIU/mL; for transabdominal USG 6500 mIU/mL).
Anembryonic gestation requires MSD of 25 mm or more without an embryo or absence of an embryo with heartbeat 2 weeks after a scan showing a sac without yolk sac. Our patient has MSD 18 mm with a visible embryo and cardiac activity — viable pregnancy. Ectopic pregnancy with pseudosac would show no yolk sac, no embryo, centrally placed fluid collection, and a single (not double) decidual ring; often a complex adnexal mass and free fluid in the cul-de-sac. Subchorionic hematoma appears as a crescentic hypoechoic collection between the chorion and decidua, often with associated threatened abortion (vaginal bleeding) — none seen here.
Teaching pearl — early pregnancy USG milestones:
| Gestation by USG | Expected finding | Beta-hCG correlation |
|---|
| 4.5-5 weeks | Gestational sac (1-2 mm), double-decidual sign | 1500-2000 mIU/mL (TVS discriminatory) |
| 5-5.5 weeks | Yolk sac inside sac (MSD over 8-10 mm) | 7,200 mIU/mL |
| 5.5-6 weeks | Embryonic pole (CRL 1-2 mm), cardiac activity | 10,800 mIU/mL |
| 6-7 weeks | CRL 5-10 mm, FHR 100-115/min | Plateaus and falls after this point |
| 8-10 weeks | Fetal movements, FHR 140-170/min | |
SRU 2013 criteria for definitive non-viable pregnancy (NEET PG favourite):
- MSD of 25 mm or more without an embryo (older cut-off was 16-20 mm; obsolete)
- CRL of 7 mm or more without cardiac activity (older cut-off was 5 mm; obsolete)
- Absence of embryo with heartbeat 2 weeks or more after a sac without yolk sac
- Absence of embryo with heartbeat 11 days or more after a sac with yolk sac
MCQ 2: 32-year-old G3P2 at 28 weeks with reduced fetal movements
Image description: [Transabdominal ultrasound of a singleton intrauterine pregnancy at apparent gestation 28 weeks by LMP. Image shows a fetus with biparietal diameter and head circumference consistent with 27-28 weeks. Fetal cardiac activity is absent on real-time M-mode imaging maintained over 5 minutes. The fetus appears flexed, with mild overlap of the fetal cranial bones (positive Spalding sign) on this multiplanar view. The amniotic fluid appears reduced (DVP 1.8 cm — oligohydramnios). Placenta posterior, no abruption. Fetal heart on real-time scan is not pulsating. Doppler in the umbilical artery shows no flow.]
Clinical vignette: A 32-year-old G3P2 woman at 28 weeks gestation (by reliable LMP and dating scan at 11 weeks) presents to the labour ward with absent fetal movements for the past 36 hours. She had felt regular movements until 2 days earlier. She has no pain, no bleeding, no fluid leakage. Past obstetric history — two uneventful term vaginal deliveries. This pregnancy has been uncomplicated; ultrasound at 19 weeks reported normal anatomy. She is otherwise healthy, non-diabetic, non-hypertensive. On examination she is hemodynamically stable; uterus consistent with 28 weeks; no tenderness; no contractions. Doppler stethoscope fails to detect fetal heart tones over multiple attempts.
Options:
- (a) Intrauterine fetal demise (IUFD) at 28 weeks
- (b) Severe fetal growth restriction with profound bradycardia
- (c) Maternal obesity obscuring fetal heart tones
- (d) Severe oligohydramnios with viable but stressed fetus
Correct answer: (a) Intrauterine fetal demise (IUFD) at 28 weeks
Reasoning: Absent fetal cardiac activity on real-time imaging maintained for 3-5 minutes, with corroborating Spalding sign (overlapping cranial bones), reduced amniotic fluid, and absent umbilical artery flow on Doppler establishes the diagnosis of intrauterine fetal demise (IUFD). At 28 weeks gestation, this fits the WHO/Indian definition of fetal death after 20 weeks (or some definitions after 28 weeks).
Severe growth restriction with bradycardia would show some cardiac activity (very slow rate of under 100/min that is still detectable on M-mode); our patient has NO cardiac activity over 5 minutes. Maternal obesity could obscure transabdominal scan but TVS or low-frequency probe would still detect activity if present. Severe oligohydramnios alone does not cause absent cardiac activity unless the fetus has demised.
Teaching pearl — diagnosis and management of IUFD:
Ultrasound criteria for IUFD:
- Primary — absent fetal cardiac activity on real-time imaging for 3-5 minutes with two observers
- Late signs (when fetal death occurred days to weeks earlier):
- Spalding sign — overlapping cranial bones (brain liquefaction)
- Robert sign — gas in fetal heart and great vessels (rare; severe)
- Deuel sign / Halo sign — fluid between fetal scalp and skull
- Exaggerated fetal spine curvature (Hartley sign)
- Macerated fetal skin (hydropic appearance)
- Reduced or absent amniotic fluid
Maternal coagulation evaluation is critical — retained dead fetus over 4 weeks releases thromboplastin and causes consumptive coagulopathy (DIC); check PT, aPTT, fibrinogen, platelets, D-dimer at diagnosis and weekly until delivery.
Management:
- Delivery recommended within 1-2 weeks of diagnosis to avoid DIC
- Mode — vaginal delivery preferred (avoids surgical morbidity in a non-life-threatening situation); LSCS only for obstetric indications
- Induction — mifepristone 200 mg PO + misoprostol 25-100 mcg vaginally or orally every 4-6 hours; or mechanical methods (Foley catheter); doses adjusted to gestational age
- Psychological support — bereavement counselling, postnatal lactation suppression, autopsy consent, RhoGAM if Rh negative
- Investigations to identify cause — fetal karyotype (cord blood, fetal cardiac blood, placental tissue), placental histopathology, TORCH screen, antiphospholipid antibody panel, maternal thrombophilia screen, glycosylated hemoglobin, autopsy when consented
MCQ 3: 35-year-old G2P1 at 32 weeks with painless vaginal bleeding
Image description: [Transvaginal ultrasound of the uterus and cervix in a 35-year-old G2P1 woman at 32 weeks gestation with painless bright red vaginal bleeding. Image shows a singleton intrauterine pregnancy with the placenta located in the lower uterine segment, completely covering the internal cervical os. The placenta extends from the anterior to the posterior lower segment, with no clear cervical visualisation between placenta and cervix. The placenta appears homogeneously echogenic with normal vasculature on colour Doppler. Cervix length is 38 mm, internal os covered by placenta. No retroplacental hematoma. Fetus active with normal cardiac activity. Amniotic fluid index normal at 14 cm.]
Clinical vignette: A 35-year-old G2P1 woman at 32 weeks gestation (previous LSCS 4 years ago for breech presentation) presents to the labour ward with a sudden onset of bright red, painless vaginal bleeding approximately 200 mL while watching television. No abdominal pain. Fetal movements normal. No leakage of fluid. On examination she is haemodynamically stable (BP 122/76, pulse 88, SpO2 99 percent); uterus is consistent with 32 weeks, soft, non-tender; no contractions. Speculum examination shows blood in the vagina, no products of conception, no obvious cervical lesion. Per vaginal examination is deferred until placenta location is confirmed.
Options:
- (a) Placenta previa (complete) on background of previous LSCS — at risk of placenta accreta spectrum
- (b) Placental abruption with concealed component
- (c) Vasa previa with sentinel bleed
- (d) Local cervical bleeding from polyp
Correct answer: (a) Placenta previa (complete) on background of previous LSCS — at risk of placenta accreta spectrum
Reasoning: Painless bright red vaginal bleeding in a third-trimester pregnancy with ultrasound showing the placenta completely covering the internal cervical os is the textbook presentation of placenta previa. The classification (RCOG 2018) is now simplified — placenta previa (covers the internal os, replaces the older "complete/partial") vs low-lying placenta (edge within 20 mm of the os but not covering, replaces the older "marginal").
This patient has additional risk factor of previous LSCS — placenta previa on a previous caesarean scar carries a 5-10 percent risk of placenta accreta spectrum (PAS) (accreta, increta, percreta). Specific PAS sonographic markers should be sought — placental lacunae (Swiss-cheese appearance), loss of the retroplacental clear space, abnormal placental-myometrial interface, bridging vessels on Doppler, placental bulge into the bladder.
Placental abruption produces painful bleeding (or concealed bleed with woody-hard tender uterus); USG may show retroplacental hematoma; here the uterus is soft and non-tender. Vasa previa produces bleeding usually at membrane rupture (sentinel bleed coincides with ROM); fetal exsanguination very rapid; colour Doppler shows vessels crossing the os. Local cervical bleeding is a diagnosis of exclusion; speculum did not show cervical lesion.
Teaching pearl — placenta previa essentials:
RCOG 2018 simplified classification:
| Classification | Definition |
|---|
| Placenta previa | Placenta covers the internal cervical os (replaces older "complete" and "partial") |
| Low-lying placenta | Placental edge within 20 mm of internal os but not covering (replaces "marginal" and old "low-lying") |
Risk factors (mnemonic ECTOPIC for placenta previa):
- Endometrial damage (previous LSCS, D&C, myomectomy)
- Caesarean section history
- Twins (large placental surface)
- Older maternal age
- Parity (multiparity)
- IVF
- Cigarette smoking
Management algorithm:
| Status | Management |
|---|
| Asymptomatic, anomaly scan reveals low placenta | Rescan at 32 weeks; 90 percent of low placentas migrate as lower segment forms |
| Asymptomatic, persistent previa at 32 weeks | Outpatient monitoring, pelvic rest, hospital admission planning, anti-D if Rh negative |
| Symptomatic, painless bleeding under 34 weeks | Admit, IV access, CBC + crossmatch 2 units, betamethasone for fetal lung maturity, magnesium sulphate for neuroprotection if under 32 weeks, expectant management if maternal-fetal stable |
| Symptomatic, painless bleeding 34-36 weeks | Admit, stabilise, consider delivery if recurrent or significant bleed |
| Definitive delivery | Elective LSCS at 36-37 weeks for placenta previa; vaginal delivery may be attempted for low-lying placenta over 20 mm from os |
| Emergency LSCS | Severe bleeding, fetal distress, maternal compromise |
Placenta accreta spectrum (PAS) red flags in placenta previa with previous LSCS:
- Multiple placental lacunae (Swiss-cheese appearance)
- Loss of normal retroplacental hypoechoic clear space
- Abnormal uteroplacental interface vascularity on colour Doppler
- Placental bulging into bladder
- Bridging vessels from placenta to bladder
- MRI for further characterisation if equivocal
- Plan delivery at tertiary centre with interventional radiology, obstetric anaesthesia, urology backup, and blood bank support
MCQ 4: 29-year-old G3P2 at 34 weeks with severe abdominal pain and minimal bleeding
Image description: [Transabdominal ultrasound of the uterus in a 29-year-old G3P2 woman at 34 weeks gestation with sudden severe abdominal pain and minimal vaginal spotting. Image shows a singleton intrauterine pregnancy with the placenta on the posterior wall. There is a focal hypoechoic to anechoic crescentic collection between the placenta and the underlying myometrium, measuring approximately 6 x 3 cm — a retroplacental hematoma. The placenta appears thickened (4.8 cm) and bulging. Amniotic fluid shows fine echoes (intra-amniotic blood). Fetal heart rate on M-mode is 110 beats per minute (bradycardia). Placental edge is well away from the internal os. The uterine wall is tense and the patient was tender on probe contact.]
Clinical vignette: A 29-year-old G3P2 woman at 34 weeks gestation, hypertensive on labetalol, presents to the labour ward with sudden severe constant abdominal pain that started 2 hours ago while walking. She has had minimal vaginal spotting (one teaspoon, dark blood). No prior trauma. Fetal movements have reduced over the past hour. On examination — BP 156/96 (raised; her usual is 130/85 on treatment), pulse 108, RR 22. Uterus is markedly tense, woody-hard, exquisitely tender, fundal height consistent with 34 weeks. CTG shows fetal bradycardia at 110/min with reduced variability. Speculum exam shows minimal blood in the vagina.
Options:
- (a) Placental abruption (revealed-and-concealed) with fetal distress
- (b) Placenta previa with concealed bleed
- (c) Uterine rupture
- (d) Severe pre-eclampsia with subcapsular liver hematoma
Correct answer: (a) Placental abruption (revealed-and-concealed) with fetal distress
Reasoning: Painful sudden-onset abdominal pain with tense woody-hard tender uterus, minimal vaginal bleeding (revealed component), fetal bradycardia (distress), background hypertension, and ultrasound showing a retroplacental hematoma with thickened placenta and intra-amniotic blood is textbook placental abruption with mixed revealed and concealed components.
Placenta previa produces painless bright red bleeding from a placenta over the os; her bleeding is minimal and the placenta is well away from the os, and the uterus would be soft and non-tender. Uterine rupture is mostly seen in previous LSCS scars or after obstructed labour; presents with sudden severe pain, loss of contractions, fetal parts palpable extra-uterine, retracting fetal heart, maternal hypotension; rare in non-scarred uterus. Severe pre-eclampsia with subcapsular liver hematoma (HELLP) presents with RUQ/epigastric pain, hypertension, proteinuria, transaminitis, thrombocytopenia, low platelets, schistocytes; uterus is not tense or tender.
Teaching pearl — placental abruption essentials:
Risk factors (mnemonic ABRUPT):
- Age (over 35 or under 20)
- Blood pressure (chronic and pregnancy-induced hypertension; commonest single risk factor)
- Ruptured membranes (sudden decompression)
- Uterine over-distension (polyhydramnios, multiple gestation)
- Previous abruption (10-fold increased risk; recurrence)
- Trauma (motor vehicle accidents, falls, domestic violence) + Tobacco/cocaine + Thrombophilia
Revealed vs concealed (NEET PG favourite):
| Feature | Revealed (80 percent) | Concealed (20 percent) |
|---|
| Vaginal bleeding | Visible, often heavy | Minimal or absent |
| Pain | Variable | Severe (rapidly expanding hematoma) |
| Uterus | Tender, may be soft initially then tense | Woody-hard, tense, exquisitely tender |
| Fetal distress | Variable, mild to severe | Severe (placental detachment is larger) |
| Maternal blood loss assessment | Easier (visible) | Underestimated (concealed) |
| Fetal mortality | 15-20 percent | 40-50 percent |
| DIC | Less common | More common (larger placental separation, more thromboplastin) |
Ultrasound caveats — sensitivity only 25-50 percent:
- Acute hematoma (under 48 hours) is hyperechoic — easily mistaken for placenta
- Subacute (3-7 days) is isoechoic
- Chronic (over 1 week) is hypoechoic
- Diagnosis is primarily clinical — do not delay management awaiting USG confirmation
Management:
| Status | Management |
|---|
| Maternal instability or fetal distress | Emergency LSCS regardless of gestation |
| Stable maternal-fetal, term or near-term (over 34 weeks) | Vaginal delivery (with continuous fetal monitoring) |
| Stable, preterm (under 34 weeks), mild abruption | Expectant management with admission, betamethasone, magnesium sulphate for neuroprotection if under 32 weeks |
| DIC | Replace clotting factors (FFP, cryoprecipitate, platelets), correct anaemia (PRC), monitor renal function |
| Anti-D | If Rh negative |
MCQ 5: 34-year-old gestational diabetic at 30 weeks with abdominal distension
Image description: [Transabdominal ultrasound of the uterus in a 34-year-old gestational diabetic woman at 30 weeks gestation, referred for fundal height greater than gestation. Image shows a single intrauterine fetus consistent in size with 30 weeks. The amniotic fluid appears markedly increased — multiple large pockets of anechoic fluid surround the fetus. Amniotic Fluid Index (AFI) is measured at 32 cm (deepest pockets in four quadrants summed). The fetus appears active. Placenta normally located anteriorly. Fetal biometry shows estimated weight on the 90th centile. Fetal stomach is visible and normal. A "double-bubble" appearance is NOT seen. No obvious anatomical anomaly on this view. There is no skin oedema or pleural effusion (no hydrops).]
Clinical vignette: A 34-year-old G2P1 woman at 30 weeks gestation with gestational diabetes (HbA1c 7.4 percent, on insulin) is referred to the OBG outpatient clinic for fundal height of 34 cm at 30 weeks gestation (greater-than-gestation). She is asymptomatic except for increasing abdominal discomfort and difficulty sleeping due to size. Fetal movements are felt as strong. No leakage, no bleeding. Past obstetric history — first child age 6, born at 38 weeks weighing 4.1 kg by normal vaginal delivery; previous gestational diabetes well-controlled.
Options:
- (a) Polyhydramnios secondary to maternal diabetes
- (b) Polyhydramnios secondary to fetal duodenal atresia
- (c) Twin pregnancy missed earlier
- (d) Macrosomia alone without polyhydramnios
Correct answer: (a) Polyhydramnios secondary to maternal diabetes
Reasoning: AFI of 32 cm at 30 weeks (over 25 cm = polyhydramnios; 30-35 cm = moderate) in a gestational diabetic with macrosomic fetus (90th centile) is textbook polyhydramnios secondary to maternal diabetes. Maternal diabetes is the commonest single identifiable cause of polyhydramnios (responsible for 20-25 percent of cases). The mechanism is fetal hyperglycaemia leading to fetal hyperinsulinaemia and resultant osmotic diuresis (fetus pees more), plus fetal-placental imbalance.
Polyhydramnios from fetal duodenal atresia would show a characteristic double-bubble sign (dilated stomach and proximal duodenum); not seen here. Twin pregnancy at 30 weeks would show two fetuses on USG; only one fetus visible. Macrosomia alone (estimated weight over 90th centile or over 4 kg) is present here but does NOT explain the AFI over 25 cm by itself.
Teaching pearl — amniotic fluid abnormalities:
Polyhydramnios — AFI over 25 cm OR DVP over 8 cm:
| Severity | AFI | DVP |
|---|
| Mild | 25-30 cm | 8-12 cm |
| Moderate | 30-35 cm | 12-16 cm |
| Severe | over 35 cm | over 16 cm |
Causes (mnemonic TRACE-PG):
- TTS — twin-to-twin transfusion syndrome (recipient twin)
- Rh isoimmunisation with hydrops
- Anomalies (fetal): oesophageal atresia, duodenal atresia (double-bubble sign), anencephaly, NTDs, congenital diaphragmatic hernia
- Cardiac fetal anomalies
- Extra (infection — TORCH, parvovirus B19)
- PATERNAL Diabetes — maternal diabetes commonest single cause
- G — idiopathic (30-40 percent; diagnosis of exclusion)
Oligohydramnios — AFI under 5 cm OR DVP under 2 cm:
Causes (mnemonic DRIPC):
- Demise of fetus
- Renal anomalies — bilateral renal agenesis (Potter sequence), posterior urethral valves (male fetus), cystic dysplasia
- IUGR — chronic placental insufficiency
- PROM — premature rupture of membranes (acute drop)
- Chronic placental insufficiency — post-term pregnancy, hypertensive disorders, abruption
Management of polyhydramnios:
- Mild-moderate, diabetic — optimise maternal glycaemic control; serial AFI monitoring; expectant management; delivery at 38-39 weeks
- Severe symptomatic — amnioreduction (1-2 L removal via needle under USG guidance; may need repeating), indomethacin in selected cases under 32 weeks (caution: ductus arteriosus closure)
- Anomaly identified — counsel; plan delivery at tertiary centre with NICU and paediatric surgery
Management of oligohydramnios:
- PROM — assess for chorioamnionitis (maternal fever, raised CRP, leukocytosis, fetal tachycardia); steroids if under 34 weeks; delivery if term or chorioamnionitis
- IUGR — uteroplacental Doppler (umbilical artery, MCA, ductus venosus); deliver if absent/reversed end-diastolic flow or ductus venosus a-wave abnormality
- Renal anomalies — counsel; Potter sequence has very poor prognosis (pulmonary hypoplasia from anhydramnios)
Common pitfalls and how to avoid them
-
Mistaking pseudosac for true gestational sac — pseudosac is centrally placed, no yolk sac, single decidual ring; true sac is eccentric, double-decidual sign, contains yolk sac.
-
Using outdated MSD and CRL cut-offs for non-viable pregnancy — older cut-offs (MSD 16 mm, CRL 5 mm) are obsolete since SRU 2013. Use MSD 25 mm and CRL 7 mm.
-
Mistaking acute retroplacental hematoma for placenta itself — acute hematoma is hyperechoic, looks like placenta. Compare with previous scans, check placental thickness (over 5 cm suspicious), look for the Kerr sign.
-
Failing to use TVS in placenta previa assessment — TVS is safe and more accurate than TAS; old fear of "probing through the placenta" is unfounded as the probe stays in the upper vagina.
-
Diagnosing placental abruption only on USG — USG sensitivity is 25-50 percent; abruption is primarily a clinical diagnosis. Do not delay management waiting for USG confirmation.
-
Not searching for PAS markers in placenta previa with previous LSCS — accreta spectrum is missed if not actively sought; plan delivery at tertiary centre with multidisciplinary team.
-
Mis-attributing polyhydramnios to "idiopathic" without ruling out diabetes and anomalies — order maternal HbA1c and OGTT; check fetal anatomy for oesophageal/duodenal atresia and neural-tube defects.
-
Using AFI only and ignoring DVP — DVP is more reliable in singleton third trimester and is the WHO-recommended single measurement; AFI cut-offs are older.
Frequently Asked Questions
What is the diagnostic ultrasound criteria for an anembryonic gestation versus a normal early pregnancy?
An anembryonic gestation (formerly blighted ovum) is diagnosed on transvaginal ultrasound when one of the SRU 2013/RCOG criteria is met. Definitive criteria for non-viable pregnancy are: mean sac diameter (MSD) of 25 mm or more with no embryo visible, OR a crown-rump length (CRL) of 7 mm or more with no cardiac activity, OR absence of an embryo with heartbeat 2 weeks or more after a scan showing a gestational sac without yolk sac, OR absence of an embryo with heartbeat 11 days or more after a scan showing gestational sac with yolk sac. A normal early intrauterine pregnancy shows an eccentric gestational sac with double-decidual sign at 4.5-5 weeks, a yolk sac inside the sac by MSD 8-10 mm (around 5.5 weeks), and a visible embryo with cardiac activity by CRL 1.5-2 mm (around 6 weeks). NEET PG often tests the MSD 25 mm and CRL 7 mm thresholds; older cut-offs (16 mm and 5 mm) are obsolete since the SRU 2013 revision.
How is intrauterine fetal demise diagnosed on ultrasound and what are the late signs?
Intrauterine fetal demise (IUFD) is defined as fetal death after 20 weeks gestation in most Indian guidelines (24 weeks in some Western standards). The primary ultrasound diagnostic criterion is absent cardiac activity on real-time imaging for at least 3-5 minutes after viable cardiac activity is expected (CRL of 7 mm or more, or after 6 weeks in any subsequent pregnancy). In early pregnancy, absent cardiac activity in an embryo with CRL of 7 mm or more is diagnostic. Other early ultrasound findings include absent fetal movements, oligohydramnios, and a flattened or collapsed fetal skull. Late signs (when fetal death occurred days to weeks earlier) include Spalding sign (overlapping cranial bones due to brain liquefaction), Robert sign (gas in the fetal heart or great vessels), Deuel sign (halo sign — fluid between fetal scalp and skull), exaggerated fetal spine curvature, and macerated fetal skin or hydrops. After diagnosis, maternal coagulation studies (PT, aPTT, fibrinogen, platelets) are essential as retained dead fetus over 4 weeks risks consumptive coagulopathy (DIC) from release of thromboplastin.
What is the classification of placenta previa and what is the management algorithm?
Placenta previa is implantation of the placenta in the lower uterine segment such that it covers or lies close to the internal cervical os. Modern (RCOG 2018) classification simplified the old four-grade system into two categories. Placenta previa: placenta covers the internal os (replaces the older complete, partial). Low-lying placenta: placental edge lies within 20 mm of the internal os but does not cover it (replaces marginal and low-lying). Diagnosis is by transvaginal ultrasound (TVS) — more accurate than transabdominal, safe even with placenta previa as the probe is inserted only into the upper vagina. Anomaly scan at 19-21 weeks identifies suspected previa; rescan at 32 weeks confirms because of placental migration (apparent shift as the lower uterine segment forms). Management depends on bleeding status and gestational age. Asymptomatic — outpatient monitoring, pelvic rest, rescan at 32-36 weeks. Symptomatic (painless bright red bleeding) — admit, IV access, group and crossmatch, IV fluids, anti-D if Rh negative, betamethasone if 24-34 weeks, expectant management. Definitive — elective LSCS at 36-37 weeks for placenta previa; vaginal delivery may be considered for low-lying placenta over 20 mm from os. Emergency caesarean for severe bleeding or fetal distress.
How does placental abruption present on ultrasound and how do concealed and revealed bleeds differ?
Placental abruption is premature separation of a normally implanted placenta before delivery — a clinical emergency. Ultrasound sensitivity is only 25-50 percent because the sonographic appearance changes with the age of the hematoma — acute blood (under 48 hours) is hyperechoic and easily mistaken for placenta, subacute (3-7 days) is isoechoic, and chronic (over 1 week) is hypoechoic. The classic finding is a retroplacental hematoma — a hypoechoic to anechoic collection between the placenta and the uterine wall. Other findings are an abnormally thickened placenta (over 5 cm), a 'jello-like' wobble on uterine pressure (positive Kerr sign), intra-amniotic blood (echoes in the amniotic fluid), and subchorionic or preplacental hematoma. Diagnosis remains primarily clinical: painful vaginal bleeding (revealed bleed, 80 percent of cases), or constant abdominal pain with woody-hard tender uterus and fetal distress with NO visible bleeding (concealed bleed, 20 percent). Concealed bleeds carry higher fetal mortality (40-50 percent) than revealed bleeds because diagnosis is delayed and blood loss is underestimated; maternal DIC risk is also higher. Management: ABC resuscitation, fetal monitoring, urgent delivery (LSCS if fetal distress or severe maternal compromise; vaginal delivery if stable maternal-fetal state and term).
What are the diagnostic criteria for polyhydramnios and oligohydramnios on ultrasound, and what are the common causes?
Amniotic fluid is assessed by two ultrasound techniques. AFI (Amniotic Fluid Index) — sum of the deepest vertical pockets in the four uterine quadrants; normal 8-25 cm at term. DVP (Deepest Vertical Pocket) — single deepest fluid pocket; normal 2-8 cm at term. Polyhydramnios is defined as AFI over 25 cm or DVP over 8 cm. Mild 25-30 cm, moderate 30-35 cm, severe over 35 cm. Causes (the mnemonic TRACE-PG): maternal diabetes (commonest, 20-25 percent), fetal anomalies (oesophageal atresia, duodenal atresia with double-bubble sign, anencephaly, neural tube defects, congenital diaphragmatic hernia — all impair fetal swallowing or absorption), twin-twin transfusion syndrome (recipient twin), Rh isoimmunisation with hydrops, infection (TORCH), idiopathic (30-40 percent). Oligohydramnios is defined as AFI under 5 cm or DVP under 2 cm. Causes (mnemonic DRIPC): demise of fetus, renal anomalies (bilateral renal agenesis = Potter sequence; obstructive uropathy from posterior urethral valves in male fetuses; cystic dysplasia), intrauterine growth restriction (IUGR — chronic placental insufficiency), premature rupture of membranes (PROM), chronic placental insufficiency (post-term pregnancy, hypertensive disorders, abruption). Management depends on cause and gestation — polyhydramnios from diabetes responds to maternal glycaemic control, severe symptomatic polyhydramnios may need amnioreduction; oligohydramnios from PROM requires assessment for chorioamnionitis and delivery, IUGR oligohydramnios needs uteroplacental Doppler and timely delivery.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026