ovarian cysts
ovarian tumors
ovarian cancer
RMI
FIGO staging
OBG
NEET PG 2026
Master ovarian cysts and tumors for NEET PG 2026 — functional cysts, benign and malignant tumors, RMI, IOTA, FIGO 2014 staging, BRCA, chemotherapy, MCQ traps.
Ovarian pathology is a NEET PG heavyweight across OBG and Pathology — expect 3 to 5 questions per paper. Lock these:
Ovarian cancer is the second-commonest gynaecological malignancy in Indian women after cervical, with an age-standardised incidence of 6.7 per 100,000 (ICMR-NCRP 2023). It is also the deadliest because 70 percent of cases present at advanced stage owing to non-specific symptoms. NEET PG examiners reach for ovarian pathology because the differential diagnosis trees are clean, the staging is surgical, and the chemotherapy regimens are well-defined.
This NEETPGAI deep dive walks through every cyst category, every tumour subtype, risk stratification with RMI and IOTA Simple Rules, FIGO 2014 surgical staging, contemporary chemotherapy, BRCA-driven risk-reducing surgery, and India-specific late-presentation challenges. Pair this guide with the PCOS deep dive for the complete adnexal-pathology map.
Functional cysts arise from the normal cyclical ovulatory process and represent the commonest "adnexal mass" encountered in reproductive-age women.
Pathology — failure of follicular rupture during ovulation; the unruptured follicle continues to grow. Lined by granulosa cells.
Size — 3 to 8 cm. Above 10 cm is rare.
Clinical — usually asymptomatic, occasionally menstrual irregularity, pelvic discomfort.
Management — observe; most resolve within 1 to 2 menstrual cycles. Repeat USG at 6 to 12 weeks. Surgery only for persistent cysts above 8 cm, suspicious features, or torsion.
Pathology — failure of corpus luteum involution after ovulation. Lined by luteinised granulosa and theca cells; haemorrhagic content common.
Clinical — delayed menses, pelvic pain, sometimes acute pain from rupture (classic mimic of ectopic pregnancy — always beta-HCG). Halban triad: amenorrhoea, abdominal pain, adnexal mass with negative HCG.
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeMaster GI secretions, digestion, absorption transporters, motility patterns, and gut hormones with high-yield NEET PG 2026 traps and India-context examples.
Master labor stages, Friedman vs Zhang curves, WHO partograph, AMTSL, episiotomy and India JSY/LaQshya policies for NEET PG 2026 OBG MCQs.
5 anterior segment ophthalmology image MCQs for NEET PG: hypopyon and Behcet, Kayser-Fleischer ring in Wilson, Brushfield spots in Down, corneal arcus, and pterygium vs pinguecula.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →Management — observe; haemodynamically stable rupture managed conservatively; emergency surgery if haemoperitoneum.
Pathology — bilateral, multilocular, large cysts caused by markedly elevated beta-HCG.
Associations — complete hydatidiform mole, choriocarcinoma, multiple gestation, ovarian hyperstimulation syndrome.
Management — resolve spontaneously after the underlying HCG-producing process is treated.
Pathology — unilocular, thin-walled cyst lined by ciliated tubal-type epithelium; clear serous fluid. Bilateral in 15 to 25 percent.
Demographics — peak age 30 to 50 years.
Treatment — cystectomy in young women, oophorectomy in older or post-menopausal.
Pathology — multilocular, large (often above 15 cm — "ovarian giant"), lined by intestinal or endocervical-type mucin-producing epithelium. Rarely bilateral (5 percent).
Complication — rupture causing pseudomyxoma peritonei (mucinous ascites — often actually appendiceal in origin).
Pathology — germ cell tumour containing tissues from all three germ layers (ectoderm dominant — hair, sebaceous material, teeth). The classic "Rokitansky protuberance" on USG.
Demographics — commonest ovarian tumour in young women (10 to 30 years).
Imaging — heterogeneous mass with hyperechoic foci (fat, calcification), shadowing tip-of-iceberg sign.
Complications — torsion (10 to 15 percent), rupture, chemical peritonitis, malignant transformation (1 percent — usually squamous cell carcinoma in postmenopausal women), infection.
Treatment — laparoscopic cystectomy preserving ovary in young women.
Pathology — rare; epithelial tumour with transitional-cell (urothelial-like) nests in fibrous stroma. Usually small, solid, unilateral, benign.
Pathology — epithelial proliferation and atypia without stromal invasion. Serous and mucinous subtypes.
Behaviour — indolent; 90 percent five-year survival even at advanced stage.
Treatment — surgical staging plus oophorectomy. Conservative fertility-sparing surgery (unilateral salpingo-oophorectomy) in young women with stage I. No adjuvant chemotherapy.
Subtypes
Risk factors — increasing age, nulliparity, early menarche, late menopause, BRCA1/2 mutation, Lynch syndrome, hormone replacement therapy, endometriosis (clear cell, endometrioid).
Protective — multiparity, breastfeeding, oral contraceptive pill (50 percent reduction after 5 years), tubal ligation, salpingectomy.
Presentation — vague abdominal bloating, early satiety, urinary urgency, pelvic pain. The "ovarian cancer symptom index" includes any of these symptoms more than 12 days per month with onset within the past year — should trigger pelvic USG and CA-125.
Affect young women (under 30 years).
Treatment — BEP chemotherapy (bleomycin, etoposide, cisplatin); fertility-sparing surgery often feasible.
| Marker | Tumour |
|---|---|
| CA-125 | Epithelial (esp. serous); also raised in endometriosis, PID, pregnancy, menstruation — limits specificity |
| HE4 | Epithelial; better specificity than CA-125 |
| AFP | Yolk sac, immature teratoma, embryonal |
| Beta-HCG | Choriocarcinoma, embryonal, dysgerminoma (occasional) |
| LDH | Dysgerminoma |
| Inhibin | Granulosa cell |
| CEA | Mucinous (also GI primary) |
| CA 19-9 | Mucinous |
| Estradiol | Granulosa, thecoma |
| Testosterone | Sertoli-Leydig |
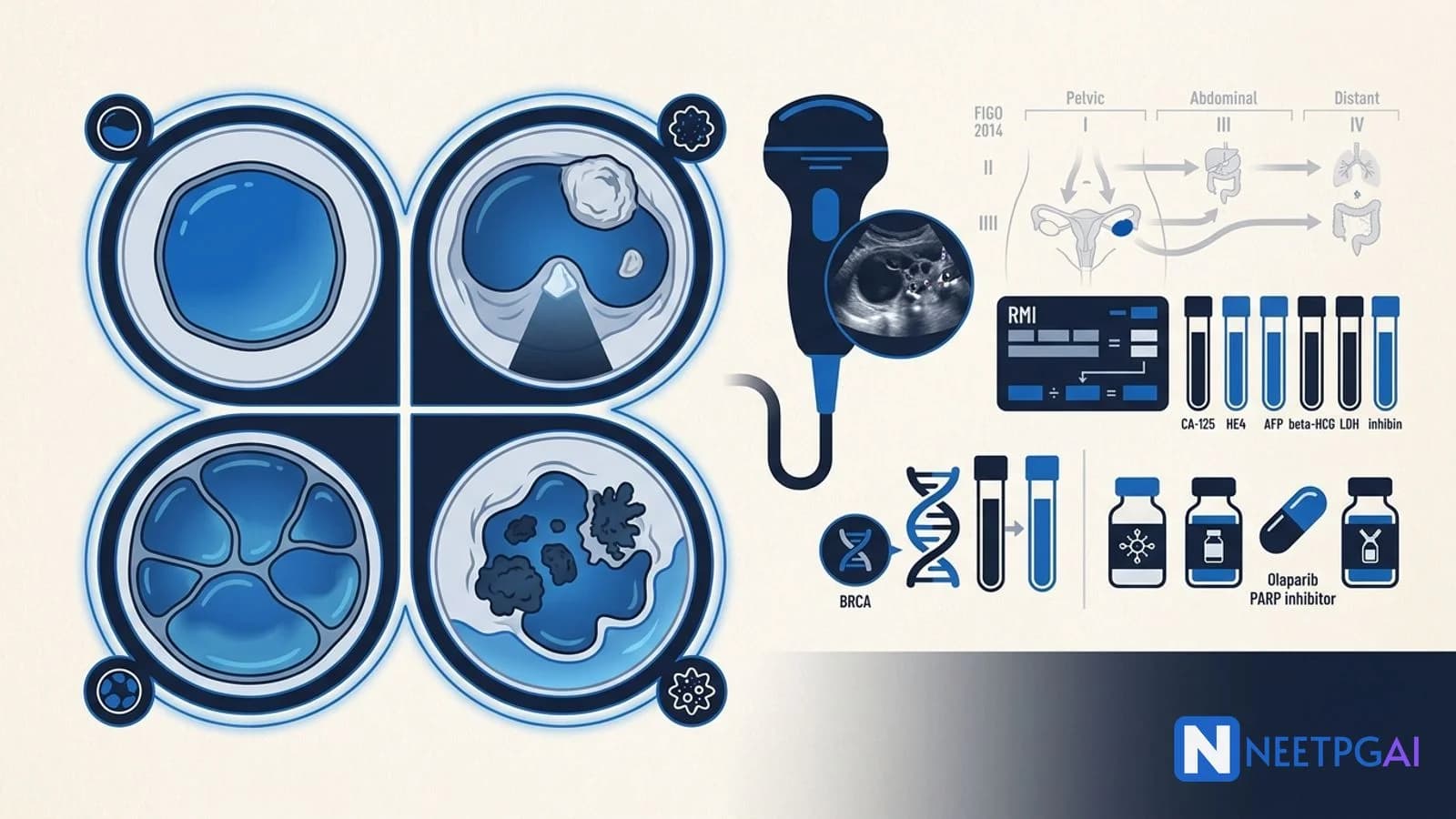
RMI = Menopausal status × Ultrasound score × CA-125 (IU/mL)
| Component | Score |
|---|---|
| Menopausal status — pre-menopausal | 1 |
| Menopausal status — post-menopausal | 3 |
| Ultrasound score — 0 or 1 feature | 1 |
| Ultrasound score — 2 or more features | 3 |
Ultrasound features: multilocular cyst, solid areas, bilateral, ascites, metastases.
RMI above 200 — refer to gynaecological oncology centre (78 percent sensitivity, 87 percent specificity).
International Ovarian Tumor Analysis group offers 5 benign (B) and 5 malignant (M) ultrasound features. If only M features are present, classify as malignant; if only B features, benign; mixed or none, indeterminate (consider MRI or refer).
| Stage | Description |
|---|---|
| I | Limited to ovaries |
| IA | One ovary, capsule intact, no malignant cells in ascites/washings |
| IB | Both ovaries, capsule intact |
| IC | IA or IB with capsule rupture (IC1 — intra-operative; IC2 — pre-operative or surface tumour; IC3 — malignant cells in ascites/washings) |
| II | Pelvic extension |
| IIA | Extension to fallopian tubes / uterus |
| IIB | Extension to other pelvic peritoneal tissues |
| III | Peritoneal spread beyond pelvis or retroperitoneal nodes |
| IIIA1 | Positive retroperitoneal nodes only |
| IIIA2 | Microscopic extra-pelvic peritoneal spread |
| IIIB | Macroscopic peritoneal metastases under 2 cm |
| IIIC | Macroscopic peritoneal metastases above 2 cm (includes liver/spleen capsule) |
| IV | Distant metastases |
| IVA | Malignant pleural effusion (cytology positive) |
| IVB | Parenchymal metastases (liver, spleen, distant nodes, extra-abdominal organs) |
Staging is surgical — exploratory laparotomy with washings, omentectomy, peritoneal biopsies, pelvic and para-aortic lymphadenectomy, total abdominal hysterectomy with bilateral salpingo-oophorectomy.
All high-grade epithelial ovarian, fallopian tube, and primary peritoneal carcinoma patients should be offered germline BRCA1/2 testing regardless of family history (NCCN 2025, ICMR 2024).
Salpingectomy at time of hysterectomy or sterilisation is now offered prophylactically given fallopian-tube origin of HGSC.
Epithelial ovarian carcinoma accounts for 90 percent of ovarian malignancies. Serous carcinoma is the commonest subtype (70 percent of epithelial), followed by mucinous, endometrioid, clear cell, and Brenner tumours. High-grade serous carcinoma carries BRCA1/2 mutations in 15 to 20 percent of cases. Median age at diagnosis is 63 years globally; presentations in India tend to be 8 to 10 years younger.
RMI is calculated as menopausal status (1 if pre-menopausal, 3 if post-menopausal) multiplied by ultrasound score (1 if 0 to 1 features, 3 if 2 or more features — multilocular, solid areas, bilateral, ascites, metastases) multiplied by serum CA-125 in IU/mL. An RMI above 200 suggests malignancy with 78 percent sensitivity and 87 percent specificity. Such patients require referral to a gynaecological oncology centre.
Meigs syndrome is the triad of a benign ovarian fibroma (sex cord stromal tumour), ascites, and right-sided pleural effusion that resolves completely after tumour resection. Pseudo-Meigs syndrome describes the same triad with other benign or malignant pelvic tumours including mucinous cystadenoma, Brenner tumour, and metastatic ovarian carcinoma — important to distinguish.
BRCA1/2 germline testing is recommended for all women with high-grade epithelial ovarian, fallopian tube, or primary peritoneal carcinoma regardless of family history (per NCCN 2025 and ICMR 2024). Carriers face 40 to 60 percent lifetime ovarian cancer risk (BRCA1) and 15 to 25 percent (BRCA2). Risk-reducing bilateral salpingo-oophorectomy at age 35 to 40 (BRCA1) or 40 to 45 (BRCA2) after childbearing is recommended.
Carboplatin plus paclitaxel every 3 weeks for 6 cycles is the global standard for adjuvant treatment of epithelial ovarian cancer (stage IC and above) after debulking surgery. PARP inhibitors (olaparib, niraparib) are added as maintenance therapy in BRCA-mutated or homologous recombination deficient tumours. Bevacizumab is added to carboplatin-paclitaxel in advanced stages. Germ cell tumours use BEP (bleomycin, etoposide, cisplatin).
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026