renal physiology
GFR
clearance
RAAS
countercurrent multiplier
physiology
NEET PG 2026
Master GFR, autoregulation, tubular reabsorption, countercurrent multiplier, RAAS, ADH, acid-base handling, and diuretic sites for NEET PG 2026 — high-yield MCQ traps.
Renal physiology contributes 3 to 5 NEET PG questions every paper across Physiology, Pharmacology, Medicine, and Anaesthesia. Lock these:
Renal physiology is one of NEET PG's stickiest topics — students under-prepare it because it feels abstract, then lose marks on clearance calculations, diuretic site-of-action questions, and acid-base puzzles that are practically free with the right framework. India-specific stems on snake-bite AKI, hot-climate volume depletion, and high CKD prevalence make it essential.
This NEETPGAI deep dive walks through nephron anatomy, GFR and autoregulation, clearance principles, segment-by-segment tubular function, the countercurrent multiplier, RAAS, ADH and aquaporins, acid-base handling, diuretic sites of action, and high-yield MCQ traps. Pair it with the acid-base disorders guide for a complete renal map.
Each kidney has about 1 million nephrons. Two types:
Functional segments — Bowman's capsule → proximal convoluted tubule (PCT) → proximal straight tubule → thin descending limb → thin ascending limb → thick ascending limb (TAL) → distal convoluted tubule (DCT) → connecting tubule → cortical collecting duct → medullary collecting duct.
Juxtaglomerular apparatus — granular (JG) cells of the afferent arteriole (renin source), macula densa of the early DCT (NaCl sensor), and extraglomerular mesangial cells.
GFR = Kf × net filtration pressure, where Kf is the filtration coefficient (surface area × hydraulic permeability).
Net filtration pressure (Starling forces) = (P-GC minus P-BC) minus (pi-GC minus pi-BC), where:
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeMaster GI secretions, digestion, absorption transporters, motility patterns, and gut hormones with high-yield NEET PG 2026 traps and India-context examples.
Master labor stages, Friedman vs Zhang curves, WHO partograph, AMTSL, episiotomy and India JSY/LaQshya policies for NEET PG 2026 OBG MCQs.
5 anterior segment ophthalmology image MCQs for NEET PG: hypopyon and Behcet, Kayser-Fleischer ring in Wilson, Brushfield spots in Down, corneal arcus, and pterygium vs pinguecula.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →Net filtration pressure approximately 10 to 17 mm Hg.
Normal GFR = 120 mL/min/1.73 m2 (180 L/day, of which 99 percent is reabsorbed).
GFR is maintained over MAP 80 to 180 mm Hg by two intrarenal mechanisms:
Clearance (C-x) = U-x × V / P-x, where U-x is urine concentration, V is urine flow rate, P-x is plasma concentration.
Inulin clearance = GFR (gold standard) — freely filtered, not reabsorbed, not secreted, not metabolised, not synthesised. Practical issue is the need for continuous IV infusion.
Creatinine clearance — practical surrogate. Overestimates GFR by 10 to 15 percent because creatinine is also secreted by the proximal tubule. Cimetidine and trimethoprim block tubular creatinine secretion → raised serum creatinine without true GFR fall.
Iohexol or 51Cr-EDTA clearance — modern gold-standard alternatives; single-injection method.
PAH clearance = renal plasma flow (RPF) — para-aminohippurate is filtered and almost completely secreted (extraction ratio 90 percent). RPF about 600 mL/min in adults.
Renal blood flow (RBF) = RPF / (1 minus hematocrit) ≈ 1100 mL/min (about 20 to 25 percent of cardiac output).
Filtration fraction (FF) = GFR / RPF = 120 / 600 = 0.2 (20 percent).
Reabsorbs about 65 percent of filtered Na+, water, Cl-, K+, and bicarbonate. Reabsorbs 100 percent of glucose and amino acids in health. Isotonic reabsorption (water follows solute).
The countercurrent multiplier.
Two cell types in the cortical collecting duct:
Acts on principal cells — increases Na+ reabsorption and K+/H+ secretion. Released in response to angiotensin II, hyperkalemia, and ACTH (minor).
Aquaporin-2 is regulated; aquaporin-3 and -4 are constitutive on basolateral side. Loss of AQP2 function or V2 mutation = nephrogenic diabetes insipidus. Lithium and demeclocycline cause acquired nephrogenic DI.
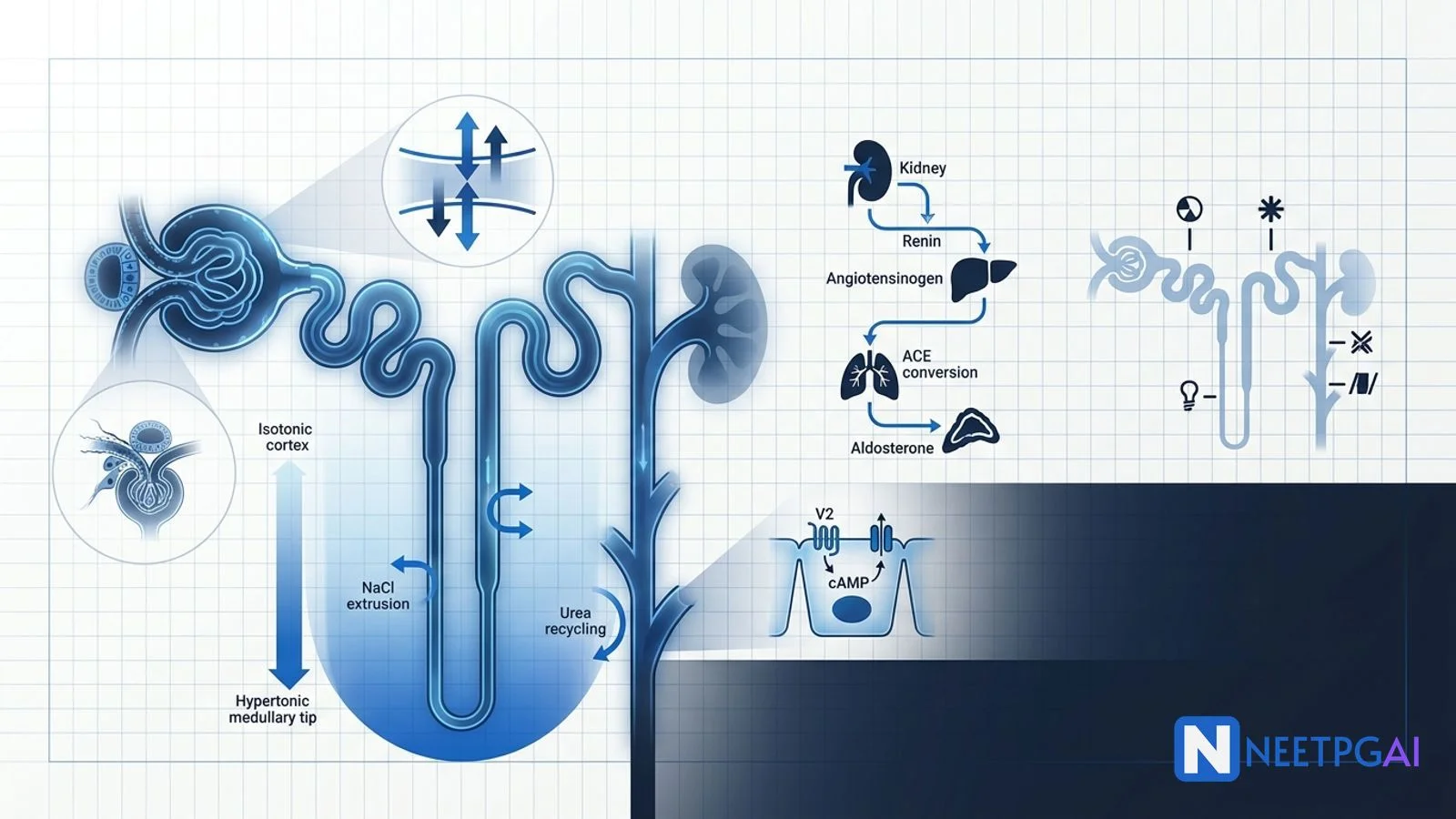
The hairpin loop of Henle creates a corticomedullary osmotic gradient (300 mOsm/L cortex to 1200 mOsm/L papillary tip).
The hypertonic medulla allows ADH-mediated water reabsorption in the collecting duct to concentrate urine to about 1200 mOsm/L. In diabetes insipidus, urine is dilute (under 300 mOsm/L) despite plasma hypertonicity.
Negative regulators — atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) suppress renin and aldosterone, promote natriuresis.
About 4500 mEq/day filtered; 85 to 90 percent reabsorbed in the PCT via the carbonic anhydrase mechanism above; the remainder in the TAL and collecting duct.
Alpha-intercalated cells secrete H+ via H+-ATPase and H+/K+-ATPase. H+ is buffered in tubular fluid by:
Net acid excretion = titratable acid plus NH4+ minus HCO3-. Normally 50 to 100 mEq/day to match endogenous acid production.
| Type | Defect | Urine pH | Serum K | Clue |
|---|---|---|---|---|
| Type 1 (distal) | Cannot secrete H+ | High (over 5.5) | Low | Calcium stones, nephrocalcinosis |
| Type 2 (proximal) | Cannot reabsorb HCO3 | Low (under 5.5) | Low | Rickets/osteomalacia, Fanconi |
| Type 4 | Aldosterone deficiency/resistance | Low | High | Diabetes, ACEi, NSAIDs |
| Diuretic class | Site | Mechanism | Key trap |
|---|---|---|---|
| Acetazolamide | PCT | Carbonic anhydrase inhibition | Metabolic acidosis, used in glaucoma, acute mountain sickness |
| Mannitol | Entire nephron (osmotic) | Osmotic diuresis | Contraindicated in anuria, heart failure |
| Loop (furosemide, bumetanide, torsemide) | Thick ascending limb | NKCC2 block | Ototoxicity, hypokalemia, hypocalcemia |
| Thiazides (HCTZ, indapamide, chlorthalidone) | DCT | NCC block | Four hypers (Ca, glucose, urate, lipid) two hypos (Na, K) |
| K-sparing (spironolactone, eplerenone) | Cortical CD | Aldosterone antagonist | Hyperkalemia, gynaecomastia (spironolactone only) |
| K-sparing (amiloride, triamterene) | Cortical CD | ENaC block | Hyperkalemia |
| Tolvaptan, conivaptan | Cortical CD | V2 antagonist | Hyponatremia (SIADH) |
| SGLT-2 inhibitors | PCT | SGLT-2 block | Glycosuria, weight loss, cardio-renal protection |
Inulin is a fructose polymer that is freely filtered at the glomerulus and is neither reabsorbed, secreted, metabolised, nor synthesised by the kidney. Its clearance therefore equals GFR exactly. Creatinine clearance overestimates GFR by 10 to 15 percent because creatinine is also secreted by the proximal tubule. Iohexol clearance is the modern practical alternative.
When GFR rises, more NaCl reaches the macula densa cells of the distal convoluted tubule. Macula densa releases adenosine, which constricts the afferent arteriole and reduces GFR back to baseline. NSAIDs blunt this by inhibiting prostaglandin-mediated afferent vasodilation — risky in volume-depleted patients.
The countercurrent multiplier is the mechanism by which the loop of Henle generates a hypertonic medullary interstitium (up to 1200 mOsm/L at the papillary tip). The thick ascending limb actively pumps NaCl out (impermeable to water), and the descending limb passively loses water (impermeable to solute). Urea recycling from the inner medullary collecting duct amplifies the gradient.
Renin is released by juxtaglomerular cells in response to three stimuli — reduced renal perfusion pressure (baroreceptor mechanism in afferent arteriole), reduced NaCl delivery to the macula densa (low intravascular volume), and beta-1 sympathetic stimulation. Renin converts angiotensinogen to angiotensin I; ACE in the lung converts angiotensin I to angiotensin II.
Thiazides block the Na-Cl cotransporter in the distal convoluted tubule. Key adverse effects — hyponatremia, hypokalemia, hypomagnesemia, hypercalcemia (paradoxical, useful in calcium stones), hyperuricemia (gout), hyperglycemia, and hyperlipidemia. The four hypers and two hypos pattern is a NEET PG favourite.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026