Quick Answer
Respiratory physiology yields 4 to 5 NEET PG questions every paper across Physiology, Medicine, Anaesthesia, and Paediatrics. Lock these:
- Lung volumes — RV, FRC, TLC need helium dilution; spirometry alone misses them.
- Oxygen dissociation curve — P50 = 27 mm Hg; CADET right shifts (raises P50).
- Dead space — anatomical (150 mL) vs physiological (anatomical plus alveolar).
- V/Q matching — apex 3.3 (high V/Q), base 0.63 (low V/Q); shunt does not correct with O2.
- CO2 transport — 70 percent as HCO3, 23 percent as carbamino, 7 percent dissolved.
- Hypoxia types — hypoxic, anemic, stagnant, histotoxic.
- PFT — FEV1/FVC under 0.70 = obstructive; raised ratio with low FVC = restrictive.
Respiratory physiology is the second densest NEET PG physiology block after cardiovascular because the oxygen-hemoglobin dissociation curve, V/Q matching, and PFT interpretation all have clean clinical correlates that examiners love. India-specific stems on high-altitude pulmonary oedema, tuberculosis-related restrictive disease, and biomass-fuel COPD push the topic even higher in yield.
This NEETPGAI deep dive walks through every lung volume and capacity, compliance and elastance, dead space, V/Q matching, the oxygen and carbon dioxide dissociation curves, Bohr and Haldane effects, hypoxia classification, work of breathing, PFT interpretation, and the chemoreceptor control of ventilation. Pair it with the cardiovascular physiology guide for a complete cardiopulmonary map.
Lung volumes and capacities
A capacity is the sum of two or more volumes. At rest in a 70 kg adult man:
| Parameter | Value | Definition |
|---|
| Tidal volume (TV) | 500 mL | Air moved per normal breath |
| Inspiratory reserve volume (IRV) | 3000 mL | Extra air inspired beyond TV |
| Expiratory reserve volume (ERV) | 1100 mL | Extra air expired beyond TV |
| Residual volume (RV) | 1200 mL | Air remaining after maximal expiration |
| Inspiratory capacity (IC) | 3500 mL | TV plus IRV |
| Functional residual capacity (FRC) | 2300 mL | ERV plus RV |
| Vital capacity (VC) | 4600 mL | IRV plus TV plus ERV |
| Total lung capacity (TLC) | 5800 mL | VC plus RV |
Cannot be measured by spirometry — RV, FRC, TLC (because each contains RV). Use helium dilution, nitrogen washout, or body plethysmography.
FRC is the resting equilibrium volume of the lung-chest system where outward chest-wall elastic recoil equals inward lung elastic recoil. It is the most important capacity clinically — it is the reservoir of oxygen between breaths and is reduced in restrictive disease and raised in obstructive disease (air-trapping).
Compliance, elastance, and surfactant
Compliance (C) = delta volume / delta pressure (units L/cm H2O). It is the ease with which the lung expands. Normal lung compliance about 0.2 L/cm H2O, chest-wall compliance similar, total respiratory system compliance about 0.1 L/cm H2O.
Elastance (E) = 1 / C — stiffness, opposite of compliance.
- Raised compliance (floppier lungs) — emphysema (loss of elastic tissue), normal aging.
- Reduced compliance (stiffer lungs) — pulmonary fibrosis, pulmonary oedema, ARDS, atelectasis, surfactant deficiency, kyphoscoliosis.
Surfactant — dipalmitoylphosphatidylcholine (DPPC) produced by type II pneumocytes from week 24, mature by week 35. Reduces surface tension at the alveolar air-liquid interface. By the Laplace law (P = 2T/r), small alveoli would empty into large ones without surfactant — leading to atelectasis and the hyaline membrane disease (neonatal RDS) seen in preterm neonates.
L/S ratio above 2 in amniotic fluid signals lung maturity; antenatal betamethasone accelerates surfactant production.
Dead space — anatomical and physiological
Anatomical dead space = volume of conducting airways not participating in gas exchange. About 150 mL in adults (about 2 mL/kg). Includes nose, pharynx, larynx, trachea, bronchi up to terminal bronchioles.
Alveolar dead space = ventilated alveoli without perfusion (e.g., pulmonary embolism). Negligible in health.
Physiological dead space = anatomical plus alveolar. Calculated by the Bohr equation — VD/VT = (PaCO2 minus PECO2) / PaCO2. PaCO2 from arterial blood, PECO2 from mixed expired gas. Normal VD/VT about 0.3.
Minute ventilation = TV × RR (e.g., 500 × 12 = 6 L/min).
Alveolar ventilation = (TV minus VD) × RR (e.g., (500 minus 150) × 12 = 4.2 L/min). Only alveolar ventilation participates in gas exchange.
V/Q matching
Ideal V/Q ratio for whole lung is about 0.8 (alveolar ventilation 4.2 L/min divided by cardiac output 5 L/min).
Regional variation in upright lung
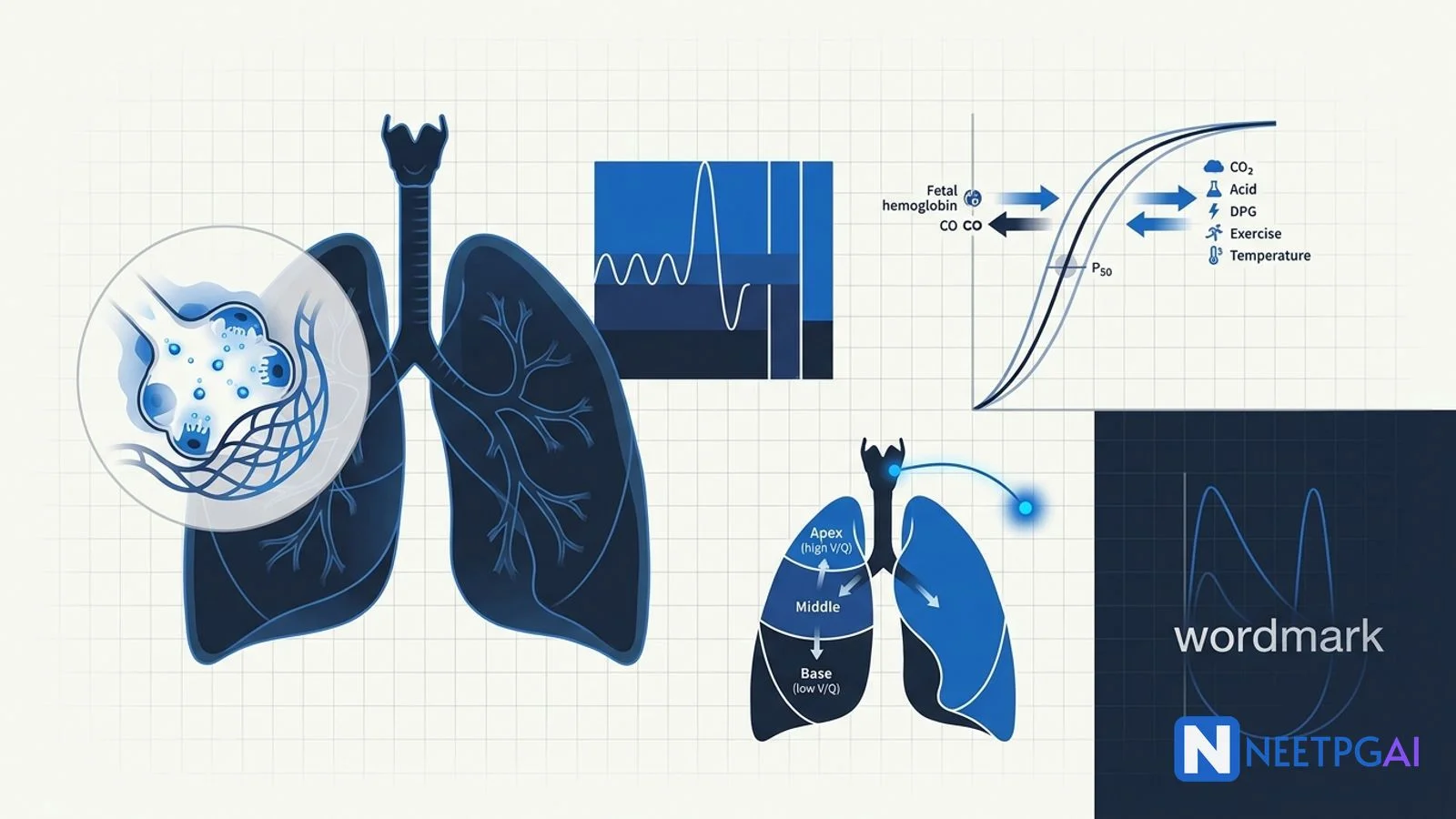
- Apex — V/Q about 3.3 (relatively underperfused due to gravity; higher PAO2, lower PACO2). Favourite site of post-primary tuberculosis.
- Base — V/Q about 0.63 (relatively overperfused; lower PAO2, higher PACO2). Favourite site of pulmonary oedema and aspiration pneumonia.
V/Q mismatch patterns
- Low V/Q (under 0.8) — perfused but underventilated. Seen in pneumonia, asthma, atelectasis, mucus plugging. Causes hypoxemia that corrects with supplemental oxygen.
- V/Q = 0 (true shunt) — no ventilation. Seen in lobar collapse, alveolar filling (severe pneumonia), intracardiac right-to-left shunt. Hypoxemia does not correct with 100 percent oxygen.
- High V/Q (over 0.8) — ventilated but underperfused. Seen in pulmonary embolism, emphysema.
- V/Q = infinity — dead space ventilation.
Hypoxic pulmonary vasoconstriction — alveolar hypoxia (low PAO2) constricts the adjacent pulmonary arteriole, diverting blood to better-ventilated alveoli. Unique to pulmonary circulation (systemic circulation vasodilates in hypoxia). Sustained global hypoxia (high altitude, COPD) causes pulmonary hypertension and cor pulmonale.
Oxygen-hemoglobin dissociation curve
The sigmoidal curve plots SaO2 (Y axis) against PaO2 (X axis). P50 is the PaO2 at which hemoglobin is 50 percent saturated — normally 27 mm Hg in adults.
Right shift (raised P50, less affinity, easier oxygen unloading at tissues) — CADET acronym
- CO2 raised
- Acid raised (lower pH) — the Bohr effect
- DPG raised (2,3-DPG, an RBC glycolytic intermediate)
- Exercise
- Temperature raised
Also: hemoglobin S, adult Hb (relative to fetal Hb).
Left shift (lower P50, more affinity, oxygen sticks to Hb at tissues) — opposite of CADET
- Low CO2, alkalosis, low 2,3-DPG (stored blood), hypothermia
- Fetal hemoglobin (HbF) — P50 about 19 mm Hg; left-shifted curve extracts O2 from maternal Hb at the placenta
- Carbon monoxide hemoglobin (HbCO) — left-shifted plus reduced O2 carrying capacity
- Methemoglobinemia (Fe3+) — left-shifted; chocolate-brown blood; treat with methylene blue
CO2 transport and the Haldane effect
CO2 is carried in three forms:
- Bicarbonate (HCO3-) — 70 percent. CO2 plus H2O → H2CO3 → HCO3- plus H+, catalysed by carbonic anhydrase in RBCs. HCO3- exits RBC via the band-3 anion exchanger in exchange for Cl- (chloride shift, Hamburger phenomenon).
- Carbamino-hemoglobin — 23 percent. CO2 binds the amino-terminal of globin chains.
- Dissolved — 7 percent.
Haldane effect — deoxygenated hemoglobin has greater affinity for CO2 and H+ than oxygenated hemoglobin. At tissues, O2 unloading allows Hb to pick up more CO2; at lungs, O2 loading releases CO2. This complements the Bohr effect — together they optimise gas exchange at both ends.
Hypoxia — four classical types
| Type | PaO2 | SaO2 | CaO2 | Mechanism | Examples |
|---|
| Hypoxic | Low | Low | Low | Low alveolar O2 or shunt | Altitude, lung disease, hypoventilation |
| Anemic | Normal | Normal/Low | Low | Reduced Hb or dysfunctional Hb | Anemia, CO poisoning, methemoglobinemia |
| Stagnant | Normal | Normal | Normal | Reduced blood flow | Heart failure, shock, vasoconstriction |
| Histotoxic | Normal | Normal | Normal | Tissues cannot use O2 | Cyanide, sepsis, mitochondrial toxin |
Cyanide poisoning — inhibits cytochrome c oxidase (complex IV); venous O2 stays high (cherry-red venous blood); treat with amyl nitrite, sodium nitrite, sodium thiosulfate, or hydroxocobalamin (preferred).
Carbon monoxide poisoning — affinity 240× greater than O2; left-shifts the curve and reduces oxygen-carrying capacity; SpO2 reads falsely normal on standard pulse oximetry (co-oximetry required); treat with 100 percent O2 (reduces half-life from 5 h to 1 h) and hyperbaric O2 for severe cases.
Work of breathing
Work = pressure × volume change. Has elastic (overcoming lung-chest recoil) and resistive (overcoming airway resistance) components.
- Restrictive disease — elastic work raised, breathe small and fast.
- Obstructive disease — resistive work raised, breathe slow and deep.
Total work is minimised at a respiratory rate of about 15/min in health, lower in restrictive and higher in obstructive disease.
Pulmonary function tests — interpretation
The single most-tested NEET PG pattern recognition exercise.
Obstructive pattern
- FEV1/FVC ratio below 0.70 (post-bronchodilator)
- FEV1 reduced disproportionately
- TLC raised (air-trapping), RV raised (hyperinflation)
- Expiratory flow-volume loop concave (scooped out)
- Reversibility (rise in FEV1 by 12 percent and 200 mL post-bronchodilator) → asthma
- DLCO reduced in emphysema, normal in chronic bronchitis and asthma
Restrictive pattern
- FEV1/FVC ratio normal or raised (above 0.70)
- Both FEV1 and FVC reduced proportionately
- TLC reduced (definitive)
- Flow-volume loop tall and narrow
- DLCO reduced in interstitial lung disease (parenchymal), normal in extrapulmonary restriction (kyphoscoliosis, neuromuscular)
Control of ventilation
Central
- Dorsal respiratory group (DRG) in medulla — inspiration; receives vagal and glossopharyngeal afferents.
- Ventral respiratory group (VRG) in medulla — active expiration during exercise.
- Pneumotaxic centre in upper pons — inhibits inspiration, increases respiratory rate.
- Apneustic centre in lower pons — promotes inspiration; lesion causes apneustic breathing (sustained inspiration).
Chemoreceptors
- Central chemoreceptors in medulla — sense CSF H+ (indirectly PaCO2 via the blood-brain barrier). Primary drive in health. Slow response (minutes). Insensitive to PaO2.
- Peripheral chemoreceptors — carotid bodies (glossopharyngeal nerve, dominant) and aortic bodies (vagus nerve). Sense PaO2 (drive only at PaO2 under 60 mm Hg), PaCO2, and pH. Fast response (seconds). The carotid body is the highest blood-flow organ per gram in the body.
In chronic CO2 retention (severe COPD), central chemoreceptors reset; hypoxic drive via peripheral chemoreceptors becomes the main driver — explaining why high-flow oxygen can suppress ventilation in advanced COPD.
Other reflexes
- Hering-Breuer — pulmonary stretch receptors inhibit inspiration at high tidal volumes; active in neonates.
- J receptors — juxtapulmonary capillary receptors; activated by pulmonary congestion, oedema, embolism; rapid shallow breathing.
NEET PG MCQ traps
- RV cannot be measured by spirometry — use helium dilution, nitrogen washout, or plethysmography.
- FRC is the resting equilibrium volume — raised in COPD (air-trapping), reduced in restrictive disease.
- CADET for right shift of O2 dissociation curve; HbF and CO shift it left.
- Bohr effect — H+ shifts curve right (oxygen unloading at tissues).
- Haldane effect — deoxy Hb carries more CO2 (CO2 unloading at lungs).
- Apex high V/Q — TB predilection; base low V/Q — pneumonia and oedema predilection.
- Shunt does not correct with 100 percent O2 — V/Q mismatch does.
- Hypoxic pulmonary vasoconstriction — unique to lung; systemic vessels vasodilate in hypoxia.
- Carotid body senses PaO2 — only kicks in below 60 mm Hg.
- Central chemoreceptors sense H+ in CSF, not direct PaCO2.
- CO poisoning — SpO2 reads falsely normal; need co-oximetry.
- Methemoglobinemia — chocolate-brown blood, treat with methylene blue.
- Cyanide — high venous O2, cherry-red venous blood, treat with hydroxocobalamin.
- L/S ratio above 2 signals fetal lung maturity.
- Type II pneumocytes make surfactant from week 24; mature week 35.
Recent updates and Indian context
- NMC CBME 2024 — emphasises mechanism-based questions on V/Q, oxygen dissociation, and PFT interpretation in respiratory physiology.
- Biomass-fuel COPD in Indian women — major cause of obstructive PFT pattern in non-smoker stems; expect spirometry interpretation paired with epidemiology.
- Tuberculosis — apical predilection driven by high V/Q and high PAO2; cavitary lesions and post-TB bronchiectasis cause mixed obstructive-restrictive PFT.
- High-altitude pulmonary oedema (HAPE) — relevant for Indian armed forces deployment; non-cardiogenic oedema from hypoxic pulmonary vasoconstriction; treatment is descent plus nifedipine plus oxygen.
Frequently asked questions
What are the lung volumes that cannot be measured by spirometry?
Spirometry cannot measure residual volume (RV), functional residual capacity (FRC), or total lung capacity (TLC) because they all include RV — the air remaining after maximal expiration. These require helium dilution, nitrogen washout, or body plethysmography. Spirometry directly measures tidal volume, inspiratory reserve volume, expiratory reserve volume, vital capacity, and inspiratory capacity.
What causes a right shift of the oxygen-hemoglobin dissociation curve?
A rightward shift means hemoglobin releases oxygen more readily at any given PaO2 — P50 rises above 27 mm Hg. Causes are remembered as the CADET acronym — raised CO2, raised acid (lower pH, the Bohr effect), raised 2,3-DPG, raised exercise/temperature. Hemoglobin S and adult Hb shift right relative to fetal Hb, which has a higher affinity for oxygen.
How do you distinguish obstructive from restrictive lung disease on PFT?
Obstructive disease (asthma, COPD) shows FEV1/FVC ratio below 0.70 with reduced FEV1, raised TLC and RV, and a concave expiratory flow-volume loop. Restrictive disease (ILD, kyphoscoliosis, obesity) shows preserved or raised FEV1/FVC ratio (above 0.70) with proportionally reduced FEV1 and FVC, reduced TLC and RV, and a narrow tall flow-volume loop. DLCO drops in emphysema and ILD.
What is V/Q mismatch and how does it cause hypoxemia?
V/Q mismatch occurs when ventilation and perfusion are unequal. Low V/Q (under 0.8) means perfused but underventilated alveoli — seen in pneumonia, atelectasis, asthma; corrects with supplemental oxygen. High V/Q (over 0.8) means ventilated but underperfused alveoli — seen in pulmonary embolism, emphysema. V/Q = 0 is true shunt (no ventilation) and does not correct with supplemental oxygen; V/Q = infinity is dead space.
What are the four types of hypoxia?
Hypoxic hypoxia — low PaO2 (high altitude, lung disease, hypoventilation). Anemic hypoxia — reduced hemoglobin or dysfunctional hemoglobin (anemia, CO poisoning, methemoglobinemia); PaO2 is normal. Stagnant (circulatory) hypoxia — reduced blood flow (heart failure, shock); PaO2 normal. Histotoxic hypoxia — tissues cannot use oxygen (cyanide, sepsis); PaO2 and SaO2 are normal, but venous O2 stays high.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026