Master AAA, aortic dissection, PAD, acute and critical limb ischaemia, and Buerger/Takayasu with thresholds, EVAR vs open, and India delays for NEET PG 2026.
Dr. NEETPGAI Editorial TeamPublished 30 May 202611 min read
Quick Answer
Vascular surgery is a 1 to 3 question topic per NEET PG paper. Lock these:
AAA elective repair — > 5.5 cm in men, > 5.0 cm in women, or rapid expansion.
Buerger disease — young male smokers; absolute cessation is the only treatment.
Takayasu arteritis — young Asian women; pulseless disease; "tree-bark" aorta.
Vascular emergencies (AAA rupture, acute aortic dissection, acute limb ischaemia) carry the highest time-to-treatment leverage in all of surgery. India also has a unique vascular epidemiology — bidi smoking driving Buerger disease, low statin coverage driving early atherosclerotic PAD, and delayed presentations to tertiary care driving high in-hospital AAA-rupture mortality. EVAR is increasingly available but cost is a barrier under PMJAY/Ayushman Bharat in many states.
This NEETPGAI deep dive walks through AAA, aortic dissection, PAD, acute and critical limb ischaemia, and the two India-relevant non-atherosclerotic arteriopathies (Buerger, Takayasu). Pair this with the head and neck cancer guide for tobacco-driven disease overlap.
Abdominal aortic aneurysm (AAA)
A true aneurysm of the infrarenal aorta — defined as > 3 cm in maximum diameter (or > 50 percent dilatation from baseline).
Epidemiology and risk factors
Age — > 65 years.
Sex — M : F = 4 : 1 (but rupture risk is higher in women size-for-size).
Smoking — strongest single modifiable risk factor (OR 5).
Hypertension, atherosclerosis, dyslipidaemia, family history.
Connective tissue disorders — Marfan, Ehlers-Danlos (more often thoracic).
Screening
A one-time abdominal ultrasound in men aged 65 to 74 (USPSTF/UK NSC). India does not yet have a national programme; opportunistic detection on CT for other indications is common.
Rupture — classical triad of sudden severe abdominal/back pain + hypotension + pulsatile abdominal mass. Retroperitoneal rupture may temporarily tamponade and present as left-flank ecchymosis (Grey-Turner sign) or hypovolaemic shock.
Share this article
Ready to put this into practice?
Start practicing NEET PG MCQs with AI-powered explanations.
Ultrasound — screening and surveillance; high specificity.
CT angiography — gold standard for sizing, anatomy, and planning repair.
In rupture — bedside USS or rapid CT if haemodynamically stable enough.
Management thresholds and modality
Diameter
Action
3.0 to 4.4 cm
USS every 12 months
4.5 to 5.4 cm
USS every 6 months
> 5.5 cm (M) or > 5.0 cm (F)
Elective repair
Rapid expansion > 1 cm/year
Elective repair (any size)
Symptomatic or ruptured
Emergency repair
EVAR vs open repair
Feature
EVAR
Open
Approach
Endovascular stent-graft via femoral arteries
Laparotomy + Dacron tube/bifurcated graft
Early mortality
Lower (1 to 2%)
Higher (3 to 5%)
Long-term mortality
Equivalent by 2 to 4 years
Lower long-term reintervention
Indication
Suitable neck/iliac anatomy, elderly/comorbid
Younger fit patients; unsuitable EVAR anatomy
Major complication
Endoleak (I-V), graft migration
Cardiac, renal, bowel ischaemia
Endoleaks — type I (attachment site, treat), type II (back-flow from lumbar/IMA — surveillance), type III (graft defect, treat), type IV (porosity, self-resolves), type V (endotension).
Thoracic aortic aneurysm (TAA)
Less common than AAA. Aetiologies skew toward connective tissue disease — Marfan, Ehlers-Danlos type IV (vascular), Loeys-Dietz — and vasculitis (Takayasu, syphilis — now rare).
Repair thresholds: ascending TAA > 5.5 cm (lower at 4.5 to 5.0 cm in Marfan), descending TAA > 6.0 cm. TEVAR (thoracic endovascular aortic repair) preferred for descending; open repair for ascending and root.
Aortic dissection
A tear in the aortic intima allows blood to dissect into the media, creating a false lumen. Mortality 1 to 2 percent per hour for untreated Stanford type A.
Classification
Stanford A — involves ascending aorta; surgical emergency.
Stanford B — involves descending aorta only; medical first.
DeBakey I — entire aorta. DeBakey II — ascending only. DeBakey III — descending only.
Clinical features
Sudden tearing chest pain radiating to the back (interscapular). May present with stroke (carotid occlusion), MI (coronary occlusion), aortic regurgitation, tamponade (type A), paraplegia (spinal artery occlusion), acute limb ischaemia, or renal failure.
Diagnosis
CT angiography — first-line in stable patients (sensitivity 100%).
TEE — for unstable patients or to assess valve and pericardium.
D-dimer — sensitive but non-specific screening.
Management
Type A — emergency surgical repair (ascending aorta graft, ± aortic valve, ± coronary reimplantation).
Type B uncomplicated — medical: beta-blocker first (esmolol/labetalol) targeting HR < 60 and SBP 100 to 120, then vasodilator (nitroprusside). Beta-blocker first to prevent reflex tachycardia.
Type B complicated (rupture, malperfusion, refractory pain) — TEVAR.
Peripheral arterial disease (PAD)
Atherosclerotic occlusive disease of lower-limb arteries. Classified by Fontaine or Rutherford stages.
Revascularisation — endovascular (angioplasty, stenting) or surgical (bypass with vein graft or PTFE) for severe claudication, rest pain, or tissue loss.
I (viable) — no immediate threat; elective revascularisation.
IIa (marginal) — salvageable with prompt treatment.
IIb (immediate) — salvageable with immediate revascularisation; sensory + motor loss.
III (irreversible) — non-viable; primary amputation.
Management — immediate IV heparin + emergent angiography → catheter-directed thrombolysis (tPA) or surgical embolectomy (Fogarty catheter). Watch for reperfusion injury and compartment syndrome (consider fasciotomy).
Critical limb ischaemia (CLI)
Chronic (> 2 weeks) rest pain or tissue loss + ABI < 0.5. Amputation risk > 30 percent at 1 year if untreated. Manage with revascularisation (endo or surgical bypass) + wound care + risk factor control.
Non-atherosclerotic arteriopathies — India focus
Buerger disease (thromboangiitis obliterans)
Demographic — young males (under 45), heavy smokers (cigarette and bidi); high prevalence in India and East Asia.
Pathology — segmental inflammatory thrombo-occlusive disease of small/medium arteries, veins, and nerves; spares macrovasculature.
Clinical — digital ischaemia, ulceration, gangrene of fingers and toes; migratory superficial thrombophlebitis (Trousseau sign — careful not to confuse with the malignancy-associated Trousseau sign).
Angiography — corkscrew collaterals around segmental occlusions; normal proximal vessels.
Treatment — absolute smoking cessation is the only effective therapy; no medication or surgical revascularisation reliably preserves limb otherwise. Iloprost may help digital ulcers.
Takayasu arteritis ("pulseless disease")
Demographic — young Asian women (under 40); high prevalence in India and Japan.
Pathology — large-vessel granulomatous arteritis of the aorta and its main branches; concentric wall thickening ("tree-bark" appearance), stenoses, occlusions, occasionally aneurysms.
Clinical — limb claudication, BP difference between arms, absent radial pulses, carotid bruit, hypertension (renal artery stenosis), aortic regurgitation, stroke.
Diagnosis — raised ESR/CRP; MR/CT angiography of aorta; ACR Numano classification (5 types by anatomical distribution).
Treatment — glucocorticoids first (prednisolone 1 mg/kg/day); methotrexate or biologics (tocilizumab) for steroid-sparing; revascularisation only during quiescent phase.
NEET PG MCQ traps
AAA size threshold for elective repair — 5.5 cm in men, 5.0 cm in women.
AAA screening — one-time USS in men 65 to 74.
EVAR endoleak types — I attachment, II IMA/lumbar back-flow, III graft defect, IV porosity, V endotension.
Stanford A dissection — surgical emergency.
Stanford B dissection — medical first (beta-blocker before vasodilator to avoid reflex tachycardia).
D-dimer — sensitive for dissection (high NPV) but non-specific.
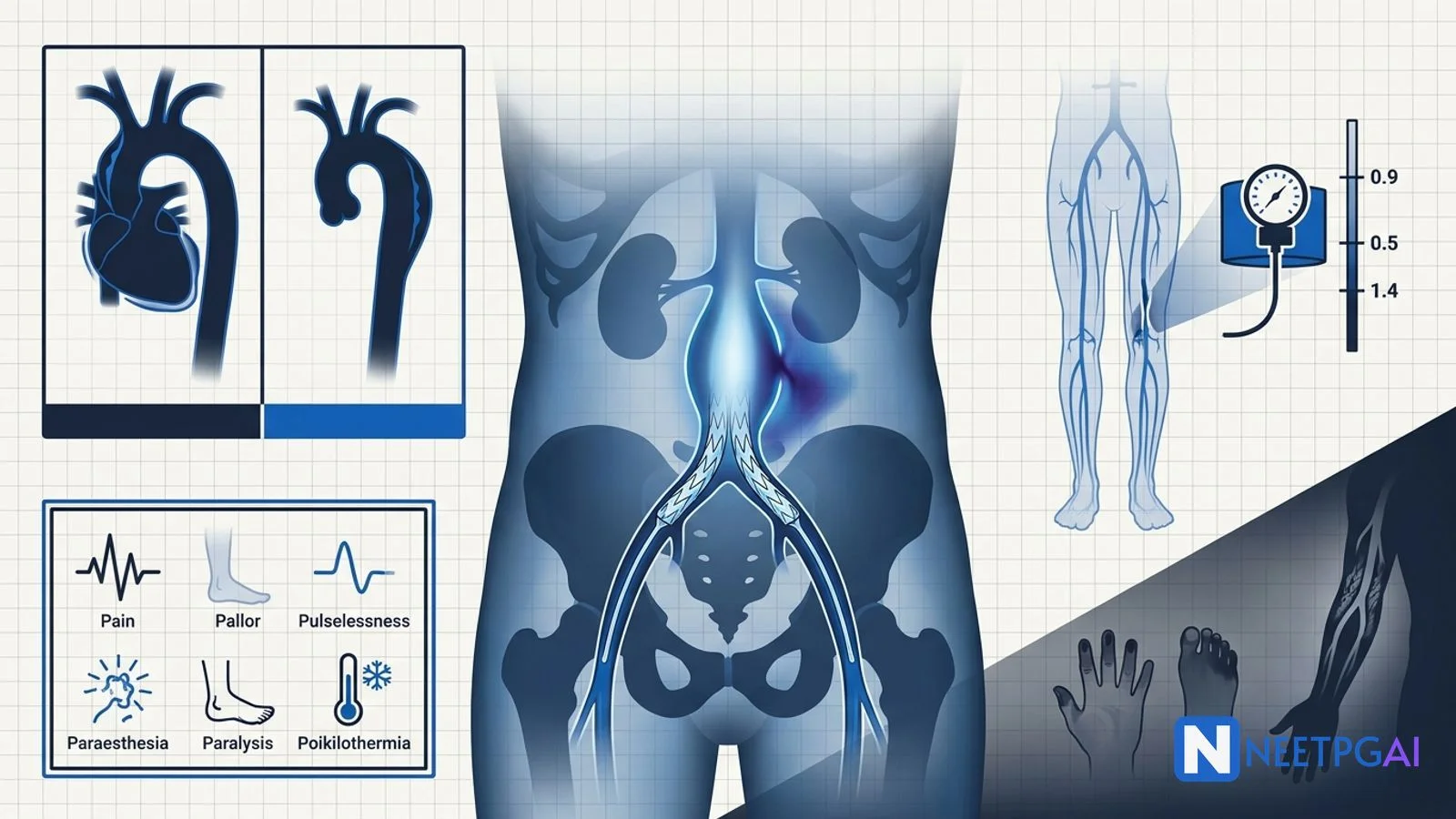
ABI — < 0.9 PAD, < 0.5 CLI, > 1.4 calcified.
Toe-brachial index — used when ABI uninterpretable (calcified vessels in diabetes/CKD); < 0.7 abnormal.
Cilostazol — PDE-3 inhibitor; first-line for claudication; contraindicated in heart failure.
Supervised exercise — most evidence-based therapy for intermittent claudication.
Rutherford IIb — immediate revascularisation; motor + sensory loss.
Compartment syndrome after revascularisation — fasciotomy (delta-pressure < 30 mmHg).
Buerger disease — young male smokers; "corkscrew" collaterals; smoking cessation only.
Takayasu — young Asian women; "tree-bark" aorta; corticosteroids first.
Trash foot — distal embolisation from a proximal AAA or atheroma.
Marfan TAA threshold — repair at 4.5 to 5.0 cm (lower than 5.5 cm general).
Most common cause of TAA today — degenerative atherosclerotic disease (not syphilis).
Recent updates and Indian context
TEVAR — now first-line for complicated type B aortic dissection (rupture, malperfusion).
EVAR availability — major Indian centres (AIIMS, PGIMER, CMC Vellore, Apollo, Fortis) routinely perform; cost ~ Rs 8 to 12 lakhs vs ~Rs 3 to 5 lakhs for open repair; PMJAY/Ayushman Bharat coverage is patchy outside empanelled centres.
Bidi smoking and Buerger — India and Bangladesh have the highest reported Buerger incidence; clusters in Punjab, UP, Bihar bidi-producing regions.
Delayed AAA-rupture presentation — Indian tertiary-care series show in-hospital mortality 40 to 60 percent vs 30 to 40 percent in high-income settings, largely due to delayed transfer.
Takayasu prevalence — India and Japan report 1 to 3 per million; ESR is normal in 50 percent of biopsy-proven cases, so imaging (MR angiography) drives diagnosis.
Frequently asked questions
When is an abdominal aortic aneurysm (AAA) repaired electively?
Elective repair of an infrarenal AAA is recommended when the maximum diameter exceeds 5.5 cm in men or 5.0 cm in women, OR when there is rapid expansion (more than 0.5 cm in 6 months or more than 1 cm/year) at any size, OR when the aneurysm becomes symptomatic (back/abdominal pain, distal embolisation). Smaller AAAs (3.0 to 5.4 cm) are surveilled with USS every 6 to 12 months. EVAR is preferred in elderly/comorbid patients with suitable anatomy; open repair offers superior long-term durability for younger patients.
How do you distinguish Stanford type A from type B aortic dissection?
Stanford classification is based on whether the ascending aorta is involved. Type A involves the ascending aorta (with or without arch/descending involvement) — a surgical emergency due to risk of aortic regurgitation, tamponade, and coronary occlusion; mortality 1 to 2 percent per hour untreated. Type B involves only the descending aorta (distal to left subclavian) — managed medically with aggressive blood pressure control (beta-blockers first, then vasodilators) unless complications develop (rupture, malperfusion, refractory pain), which mandate TEVAR.
What is the ankle-brachial index (ABI) and how is it interpreted?
The ankle-brachial index is the ratio of the higher of dorsalis pedis or posterior tibial systolic pressure to the higher brachial systolic pressure. Normal is 1.0 to 1.4. ABI under 0.9 confirms peripheral arterial disease (PAD); 0.5 to 0.9 indicates claudication; under 0.5 indicates critical limb ischaemia. ABI over 1.4 suggests non-compressible calcified vessels (diabetes, CKD) — use toe-brachial index (under 0.7 abnormal) instead. ABI is the cheapest, most reproducible, and most sensitive bedside vascular screen.
What are the 6 Ps of acute limb ischaemia?
Acute limb ischaemia presents with the classic 6 Ps — Pain (sudden, severe), Pallor (early), Pulselessness (distal to occlusion), Paraesthesia (early sensory loss), Paralysis (late motor loss), and Poikilothermia (cold limb). Onset under 14 days defines acute. Time-to-revascularisation determines limb salvage — irreversible muscle necrosis at 6 to 8 hours. Rutherford classification (I viable, IIa marginal, IIb immediate threat, III irreversible) guides urgency. IIa to IIb need emergent angiography + catheter-directed thrombolysis or surgical embolectomy.
What is Buerger disease and how is it managed?
Buerger disease (thromboangiitis obliterans) is a non-atherosclerotic, segmental, inflammatory thrombo-occlusive disease of small and medium arteries, veins, and nerves. It affects young (under 45) male heavy smokers, classically the digital arteries of the hands and feet (digital ischaemia, gangrene, migratory superficial thrombophlebitis). India has a high incidence in bidi smokers. Diagnosis is clinical (Shionoya criteria) — corkscrew collaterals on angiography. The ONLY effective treatment is absolute smoking cessation; no medication or revascularisation reliably preserves limb otherwise.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: May 2026