mistake guide
orthopedics
fractures
Salter Harris
compartment syndrome
DDH
Gustilo Anderson
Avoid the costliest orthopedic mistakes in NEET PG 2026: Colles vs Smith, Salter-Harris, fracture healing, dislocations, RA vs OA, septic arthritis, compartment syndrome, AVN, DDH, Gustilo.
Version 1.0 — Published May 2026
Orthopedics contributes 8-12 questions in NEET PG, often coupled with radiology and rheumatology. The 14 most expensive mistakes cluster around fracture eponyms, paediatric growth plate injuries, joint pathology, and orthopedic emergencies. To protect your marks:
Orthopedics sits at the intersection of surgery, radiology, paediatrics, and rheumatology. A single misclassified Salter-Harris or missed compartment syndrome on an MCQ can cost 1-2 marks; in practice, missing the diagnosis means lifelong disability or limb loss. NEET PG and INI-CET examiners use orthopedic vignettes to test pattern recognition (eponyms, classifications), emergencies (compartment syndrome, fat embolism, open fractures), and high-yield trivia (AVN sites, Gustilo classification).
The 14 mistakes below come from analysis of NEET PG 2019-2024 orthopedics questions and represent the most frequent error patterns. Pair this guide with the bone X-ray pathology image MCQ for deeper imaging coverage.
What students do: Memorise both as "distal radius fracture" without locking in the displacement direction.
Start practicing NEET PG MCQs with AI-powered explanations.
Start Free PracticeMaster GI secretions, digestion, absorption transporters, motility patterns, and gut hormones with high-yield NEET PG 2026 traps and India-context examples.
Master labor stages, Friedman vs Zhang curves, WHO partograph, AMTSL, episiotomy and India JSY/LaQshya policies for NEET PG 2026 OBG MCQs.
5 anterior segment ophthalmology image MCQs for NEET PG: hypopyon and Behcet, Kayser-Fleischer ring in Wilson, Brushfield spots in Down, corneal arcus, and pterygium vs pinguecula.
Daily MCQs, study tips, and topper strategies on Telegram.
Join on Telegram →Why it is wrong: NEET PG specifically asks about displacement direction and deformity name. Calling a volar-displaced fracture "Colles" is a one-mark loss.
Correct approach:
| Feature | Colles | Smith (reverse Colles) |
|---|---|---|
| Displacement | DORSAL (posterior) | VOLAR (anterior) |
| Angulation | Dorsal | Volar |
| Deformity | Dinner-fork on lateral view | Garden-spade on lateral view |
| Mechanism | FOOSH with wrist extended | Fall on flexed wrist; backward fall with hand behind |
| Frequency | Common — elderly osteoporotic women | Less common |
| Associated | Ulnar styloid fracture (60 percent), median nerve injury | Median nerve injury |
| Management | Closed reduction + below-elbow cast in slight palmar flexion and ulnar deviation; ORIF if unstable/intra-articular | Closed reduction + cast in dorsiflexion; ORIF often required (Smith is more unstable) |
Other distal radius eponyms:
How to remember: Colles = Dorsal (both end in -s); Smith = Volar (Smith has a "V" sound). Or visually: Colles produces a dinner-fork (dorsal hump), Smith produces a garden-spade (volar bulge).
What students do: Remember only Type II (the commonest) and confuse the others.
Why it is wrong: Each Salter-Harris type has different prognosis and management. Calling a Type III "Type II" misses the intra-articular nature and the need for anatomical reduction.
Correct approach — SALTR mnemonic:
| Type | Mnemonic | Description | Prognosis | NEET PG pearl |
|---|---|---|---|---|
| I | S — Slipped/Straight | Pure transverse fracture through physis | Good | Young children; may need wide physeal X-ray view |
| II | A — Above | Through physis extending UP into metaphysis | Good | MOST COMMON (75 percent); Thurston-Holland fragment in metaphysis |
| III | L — Lower | Through physis extending DOWN into epiphysis | Moderate (intra-articular) | Requires anatomical reduction; risk of growth arrest |
| IV | T — Through/Together | Through metaphysis AND epiphysis, crossing physis | Worse | Requires anatomical reduction (often ORIF); high growth arrest risk |
| V | R — Rammed/Ruined | Crush injury to physis | Worst | Often missed initially; growth arrest, limb shortening, angular deformity |
How to remember: SALTR, with the action progressing from PURE physis (I) → up into metaphysis (II) → down into epiphysis (III) → through both (IV) → ruined/crushed (V).
Key principle: Anatomical reduction is essential for Types III and IV (intra-articular); growth-arrest follow-up is essential for Types III, IV, and V. Always document neurovascular status and document the type clearly on imaging reports.
What students do: Mix up the order or compress 5 stages into "callus formation".
Why it is wrong: NEET PG asks "at what stage is callus visible on X-ray" — soft callus at 2-3 weeks, hard callus at 6-12 weeks. Getting the sequence wrong costs the question.
Correct sequence — 5 stages:
| Stage | Timing | Key event |
|---|---|---|
| 1. Hematoma formation | 0-72 hours | Bleeding from disrupted vessels forms a fibrin-rich clot at fracture site |
| 2. Inflammation | 1-7 days | Macrophages and inflammatory cells clear debris; release of cytokines (TNF, IL-1, IL-6, BMP) recruits stem cells |
| 3. Soft callus (fibrocartilaginous) | 2-3 weeks | Mesenchymal stem cells differentiate into chondroblasts and fibroblasts; cartilage and fibrous tissue bridge the gap; visible on X-ray |
| 4. Hard callus (bony) | 6-12 weeks | Endochondral ossification converts cartilage to woven bone; visible callus on X-ray with bridging |
| 5. Remodeling | Months to years | Woven bone is replaced by lamellar bone; restoration of medullary cavity; Wolff's law — bone remodels along lines of stress |
Two types of bone healing:
How to remember: "Hematoma → Inflammation → Soft callus → Hard callus → Remodeling" — mnemonic "HISHR" or simply visualise the timeline (days → weeks → months → years).
What students do: Use these terms interchangeably.
Why it is wrong: Each has a specific meaning and different management. NEET PG tests vocabulary directly.
Correct definitions:
Common dislocations:
What students do: Memorise RA vs OA in isolation without integrating distribution, morning stiffness, and X-ray findings.
Why it is wrong: NEET PG vignettes often give partial features; only the integrated pattern recognition gets the answer.
Correct approach:
| Feature | Rheumatoid arthritis (RA) | Osteoarthritis (OA) |
|---|---|---|
| Joints involved | MCP, PIP, wrist (symmetric small joints first) | DIP, CMC of thumb, knee, hip, spine (large weight-bearing joints) |
| Distribution | Symmetric, polyarticular | Asymmetric, oligoarticular |
| Morning stiffness | Over 1 hour, worsens with rest, improves with use | Under 30 min, worsens with use, improves with rest |
| Systemic features | Fatigue, weight loss, fever, extra-articular (nodules, vasculitis, pleuritis, episcleritis) | None |
| Lab findings | Raised ESR/CRP, RF positive (70-80 percent), anti-CCP positive (more specific) | Normal labs |
| X-ray findings | Periarticular osteopenia, joint space narrowing (uniform), marginal erosions, ulnar deviation, swan-neck/boutonnière deformities | Joint space narrowing (asymmetric/non-uniform), osteophytes, subchondral sclerosis, subchondral cysts, Heberden (DIP) and Bouchard (PIP) nodes |
| Synovial fluid | Inflammatory (WBC 5,000-50,000, mostly neutrophils early then mixed) | Non-inflammatory (WBC under 2,000, mostly mononuclear) |
| Treatment | DMARDs (methotrexate first-line), biologics (anti-TNF, anti-IL-6, JAK inhibitors), steroids for flares | Analgesics, NSAIDs, physiotherapy, intra-articular steroids, joint replacement |
How to remember:
The classic exam trap: a vignette with DIP involvement and Heberden's nodes is OA, NOT RA. RA typically SPARES the DIP joints.
What students do: Both have fever and joint pain — call both "septic".
Why it is wrong: Septic arthritis is a surgical emergency requiring joint aspiration and antibiotics within 24 hours. Missing it destroys the joint.
Correct approach:
| Feature | Septic arthritis | Reactive arthritis |
|---|---|---|
| Pathophysiology | Direct infection of joint (haematogenous, contiguous, or iatrogenic) | Sterile inflammation triggered by extra-articular infection (post-Chlamydia, post-Salmonella/Shigella/Yersinia gastroenteritis) |
| Onset | Acute (hours to days), hot/red/swollen single joint | Days to weeks after triggering infection |
| Joint distribution | Monoarticular usually; knee most common in adults, hip in children | Asymmetric oligoarthritis (knees, ankles, sacroiliac); enthesitis |
| Fever | Often high | Mild or absent |
| Synovial fluid WBC | Over 50,000 (often over 100,000), mostly neutrophils, low glucose, positive Gram stain/culture in 50-70 percent | 2,000-50,000, sterile culture |
| Causative organism | Adults: S. aureus (commonest), Streptococcus, Gonococcus (young sexually active); Children: S. aureus, Kingella kingae (under 4 yr); IVDU/elderly: Gram-negatives | None in joint; trigger organisms identified by stool culture, urine PCR, urethral swab |
| Associated features | None typically | Conjunctivitis, urethritis (Reiter triad), keratoderma blennorrhagicum, circinate balanitis, HLA-B27 positive |
| Treatment | Emergency joint aspiration + IV antibiotics (empirical: ceftriaxone + vancomycin, adjust to culture; duration 2-4 weeks IV then oral) + arthroscopic/open washout | NSAIDs, intra-articular steroids; treat triggering infection with antibiotics; biologics for chronic disease |
Key principle: ANY child or adult with monoarticular hot joint + fever must have urgent joint aspiration to rule out septic arthritis. Kocher criteria for paediatric septic hip: fever over 38.5 C, non-weight-bearing, ESR over 40, WBC over 12,000 — 3-4 criteria predict over 90 percent risk of septic arthritis.
What students do: Wait for the classic 5 P's including pulselessness to make the diagnosis.
Why it is wrong: Pulses are typically PRESENT in early compartment syndrome (compartment pressure rarely exceeds systolic BP). Waiting for pulselessness means muscle and nerve are already irreversibly damaged. Pain out of proportion is the earliest sign.
Correct approach — 5 P's, in order of appearance:
A 6th P (Poikilothermia/cold) is sometimes added.
Diagnostic threshold:
Treatment: emergency fasciotomy within 6 hours. Delayed fasciotomy causes irreversible muscle necrosis, contracture (Volkmann ischaemic contracture in forearm; clawing of fingers/toes), and rhabdomyolysis with AKI. After fasciotomy, leave wound open and close after 5-7 days when swelling subsides.
Commonest sites:
Risk factors: tibial shaft fracture (most common), supracondylar humerus fracture, crush injury, prolonged compression, tight cast/dressing, severe burns, snakebite, IV extravasation, reperfusion after vascular surgery.
What students do: Attribute hypoxia and confusion in a polytrauma patient to PE or sepsis.
Why it is wrong: Fat embolism syndrome (FES) has a specific triad and a specific window (24-72 hours after long-bone fracture). Treatment is supportive and prevention is fracture stabilisation.
Correct approach — Gurd's criteria for FES:
Major criteria:
Minor criteria: tachycardia, fever, retinal changes (Purtscher retinopathy — cotton-wool spots), jaundice, renal changes, thrombocytopenia, anaemia, raised ESR, fat globules in sputum/urine.
Diagnosis: ≥1 major + ≥4 minor criteria, or 2 major criteria.
Timing: 24-72 hours after long-bone fracture (commonly femur), polytrauma, or pelvic surgery.
Pathophysiology:
Treatment:
Mortality: 5-15 percent if recognised; higher if missed.
What students do: Apply adult fracture morphology to paediatric vignettes.
Why it is wrong: Paediatric bones are more elastic, periosteum is thicker, and growth plate adds vulnerability. Distinct fracture patterns occur.
Correct paediatric fracture types:
Key principle: Paediatric remodelling is excellent — even moderate angulation in young children remodels over time (especially in the plane of joint motion). But rotational deformity does NOT remodel — must be corrected.
What students do: Treat these as variants of the same word.
Why it is wrong: They are completely different entities. NEET PG examiners use the names interchangeably to trap.
Correct definitions:
Mnemonic: Lysis = lesion (pars defect); Listhesis = lateral/forward slip; Sis (osis) = arthritis.
What students do: Confuse which test is for relocation vs provocation.
Why it is wrong: NEET PG examiners directly test the direction of force and the meaning of a positive sign.
Correct approach:
| Test | Action | Positive sign meaning |
|---|---|---|
| Ortolani (relocation) | Hip ABDUCTED, greater trochanter LIFTED ANTERIORLY | Palpable CLUNK as dislocated hip relocates → dislocated but reducible |
| Barlow (provocation) | Hip ADDUCTED, knee pushed POSTERIORLY | Palpable clunk as hip dislocates posteriorly → dislocatable (unstable) |
Important: A "click" (high-pitched, soft tissue) is NOT pathological — a "clunk" (low-pitched, mechanical, palpable) is. Distinguishing click from clunk takes practice.
Limitations: Both tests become less reliable after 3 months as soft-tissue contractures develop. After 3 months, look for:
Imaging:
Risk factors for DDH: Female sex (4-6x), breech presentation, family history, firstborn, oligohydramnios, swaddling with hips extended, postural deformity.
Treatment:
What students do: Forget which bones are at high risk of avascular necrosis after fracture.
Why it is wrong: AVN is a delayed complication with specific anatomical predispositions. NEET PG asks "which fracture has highest risk of AVN" — the answer depends on knowing the blood supply.
Correct list — AVN-prone sites and why:
Risk factors for non-traumatic AVN: Steroid use (long-term), alcohol, sickle cell disease, lupus, antiphospholipid syndrome, Gaucher disease, decompression sickness (dysbaric osteonecrosis), pregnancy, idiopathic.
Imaging: MRI is the gold standard — shows marrow edema and the characteristic "double-line sign" or "crescent sign" early, before X-ray changes appear.
Ficat-Arlet staging of femoral head AVN:
Treatment: Core decompression for early stages; bone grafting; osteotomy; hip replacement for advanced disease.
What students do: Use "open fracture" as a single category and miss the gradation.
Why it is wrong: Gustilo-Anderson classification guides antibiotic regimen, soft-tissue management, and prognosis. Examiners ask which grade requires which antibiotic.
Correct classification:
| Grade | Wound size | Soft-tissue injury | Contamination | Antibiotic |
|---|---|---|---|---|
| I | Under 1 cm | Minimal | Clean | Cefazolin (1st-gen cephalosporin) |
| II | 1-10 cm | Moderate | Moderate | Cefazolin |
| IIIA | Over 10 cm | Extensive but adequate soft-tissue coverage available | Heavy | Cefazolin + aminoglycoside (gentamicin) |
| IIIB | Over 10 cm | Extensive with periosteal stripping, requires flap | Heavy | Cefazolin + aminoglycoside; consider piperacillin-tazobactam |
| IIIC | Any | Associated arterial injury requiring repair | Variable | Cefazolin + aminoglycoside; consider piperacillin-tazobactam; emergency vascular surgery |
Additional considerations:
Outcomes: IIIB-IIIC have substantially higher rates of infection (15-25 percent), non-union, and amputation (especially IIIC with limb-salvage failure).
MESS (Mangled Extremity Severity Score) ≥7 traditionally predicted amputation in lower limbs with vascular injury; modern data show many limbs with MESS 7-9 can be salvaged with modern microsurgery — score is no longer a strict amputation threshold but informs counselling.
What students do: Jump to "ORIF" without thinking through the conservative principles.
Why it is wrong: Most fractures are managed by the 3 Rs in a stepwise manner. NEET PG examiners test the conceptual framework.
Correct approach — the 3 Rs of fracture management:
Reduction — restoring anatomical alignment
Retention (immobilisation) — maintaining reduction during healing
Rehabilitation — restoring function
Key principle: "Move what you can, don't move what you cannot" — early mobilisation of uninjured joints prevents stiffness; the fractured segment requires immobilisation appropriate to its stability.
The 14 most cost-effective mistakes to fix:
Master these 14 patterns and you protect ~10 marks across orthopedic, radiology, and rheumatology questions in NEET PG 2026.
Orthopedics contributes 8-12 questions per NEET PG paper (2021-2024 paper analysis), including overlap with surgery, radiology, and rheumatology. Question themes cluster around fracture eponyms (Colles, Smith, Monteggia, Galeazzi, Bennett, Boxer's, Jones), Salter-Harris classification, dislocations, paediatric orthopedics (DDH, Perthes, slipped capital femoral epiphysis), compartment syndrome, fat embolism, septic vs reactive vs RA vs OA arthritis, AVN sites, open fracture Gustilo-Anderson classification, spinal disorders (spondylolisthesis, spondylolysis, ankylosing spondylitis), and bone tumours. The 14 mistakes in this guide cover roughly 60-70 percent of typical orthopedic question failures.
Both are distal radius fractures within 2.5 cm of the wrist joint, but with opposite displacement directions. Colles fracture: extra-articular distal radius fracture with DORSAL (posterior) displacement and DORSAL angulation of the distal fragment, producing the classic 'dinner-fork' deformity on lateral view. Mechanism: fall on outstretched hand (FOOSH) with wrist in extension. Commonest in elderly women with osteoporosis. Often associated ulnar styloid fracture (60 percent). Smith fracture (reverse Colles): extra-articular distal radius fracture with VOLAR (anterior) displacement and VOLAR angulation of the distal fragment, producing a 'garden-spade' deformity on lateral view. Mechanism: fall on flexed wrist or backward fall with hand behind. Less common than Colles. Both are typically managed with closed reduction and below-elbow plaster cast; surgical fixation (volar plate or K-wires) for unstable, intra-articular, or significantly displaced fractures, particularly in younger active patients.
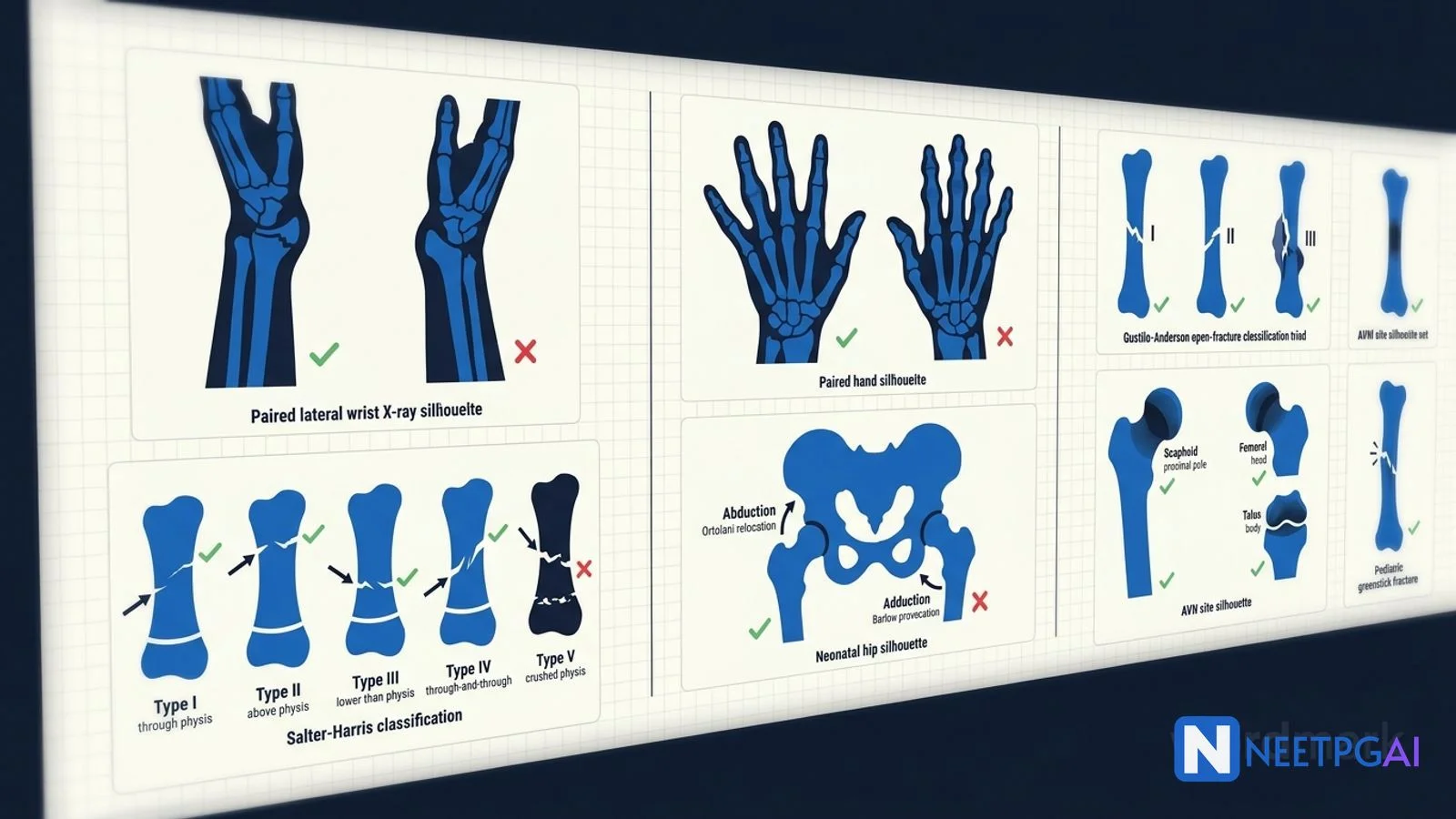
The Salter-Harris classification (1963) describes fractures involving the physis (growth plate) in skeletally immature children. Five types — mnemonic SALTR. Type I (S — Slipped/Straight): fracture purely through the physis, no metaphyseal or epiphyseal involvement; typically in young children; good prognosis; can be difficult to see on X-ray (look for widened physis). Type II (A — Above): fracture through the physis extending up into the metaphysis (a triangular metaphyseal fragment called the Thurston-Holland fragment is the key X-ray sign); MOST COMMON type (75 percent of all Salter-Harris); good prognosis. Type III (L — Lower): fracture through the physis extending down into the epiphysis (joint surface); intra-articular, requires anatomical reduction; risk of growth arrest. Type IV (T — Through/Together): fracture through both the metaphysis AND the epiphysis crossing the physis; intra-articular, requires anatomical reduction; high risk of growth arrest. Type V (R — Rammed/Ruined): crush injury to the physis; often missed on initial X-ray; worst prognosis with growth arrest and limb-length discrepancy. Higher types (III-V) have higher risk of premature physeal closure and require careful follow-up.
Compartment syndrome is increased pressure within a closed fascial compartment that exceeds capillary perfusion pressure, leading to ischaemic muscle and nerve necrosis. The classic 5 P's are: Pain out of proportion to injury (the EARLIEST and most sensitive sign — pain on passive stretch of the involved muscles is highly characteristic), Pallor, Paraesthesia, Paralysis (LATE), Pulselessness (VERY LATE — if pulses are absent, severe ischaemia has already occurred). A 6th P (Poikilothermia) is sometimes added. Pulses are typically PRESENT in early compartment syndrome because compartment pressure rarely exceeds systolic blood pressure — DO NOT wait for pulselessness. Diagnosis: clinical with high suspicion. Compartment pressure measurement (Stryker needle) is confirmatory — absolute compartment pressure over 30 mmHg OR delta pressure (diastolic BP minus compartment pressure) under 30 mmHg is diagnostic. Treatment: EMERGENCY fasciotomy within 6 hours — this is a limb-saving emergency. Commonest sites: leg (anterior compartment with deep peroneal nerve, posterior compartment with tibial nerve), forearm (Volkmann ischaemic contracture if missed).
Both are neonatal physical examination manoeuvres to detect developmental dysplasia of the hip (DDH, previously congenital dysplasia of hip) — performed in newborns before discharge and at 6-week well-baby check. ORTOLANI test (relocation): with the baby supine, hips and knees flexed to 90 degrees, the examiner's middle finger placed over the greater trochanter and thumb on the medial thigh, the hip is ABDUCTED while the greater trochanter is lifted ANTERIORLY — a palpable CLUNK (not click) as the dislocated femoral head relocates into the acetabulum is a positive Ortolani sign, indicating a DISLOCATED but reducible hip. BARLOW test (provocation, opposite direction): with the same starting position, the hip is gently ADDUCTED while applying POSTERIOR pressure on the knee — a palpable clunk as the femoral head dislocates posteriorly out of the acetabulum is a positive Barlow sign, indicating a DISLOCATABLE (unstable) but currently located hip. Both tests become less reliable after 3 months as soft-tissue contractures develop. After 3 months, the screening tests are limited abduction (under 60 degrees, asymmetric), Galeazzi sign (apparent femoral shortening on one side when knees are flexed), and asymmetric thigh creases. Imaging: ultrasound is the investigation of choice from birth to 6 months (Graf alpha angle, Harcke dynamic technique); X-ray pelvis AP is used after 6 months when the femoral head has ossified (Acetabular index, Shenton's line, Hilgenreiner's line, Perkin's line).
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team Reviewed by: Pending SME Review Last reviewed: May 2026