Quick Answer
Hepatobiliary cancer delivers 2 to 3 NEET PG questions per year across medicine, surgery and radiology. Lock these:
- HCC risk — HBV (India leader) > HCV > NAFLD > alcohol > aflatoxin.
- HCC screening — cirrhotic patients need AFP + USG every 6 months.
- LI-RADS 5 — arterial hyper-enhancement + washout on 4-phase CT/MRI → diagnostic without biopsy in cirrhotic.
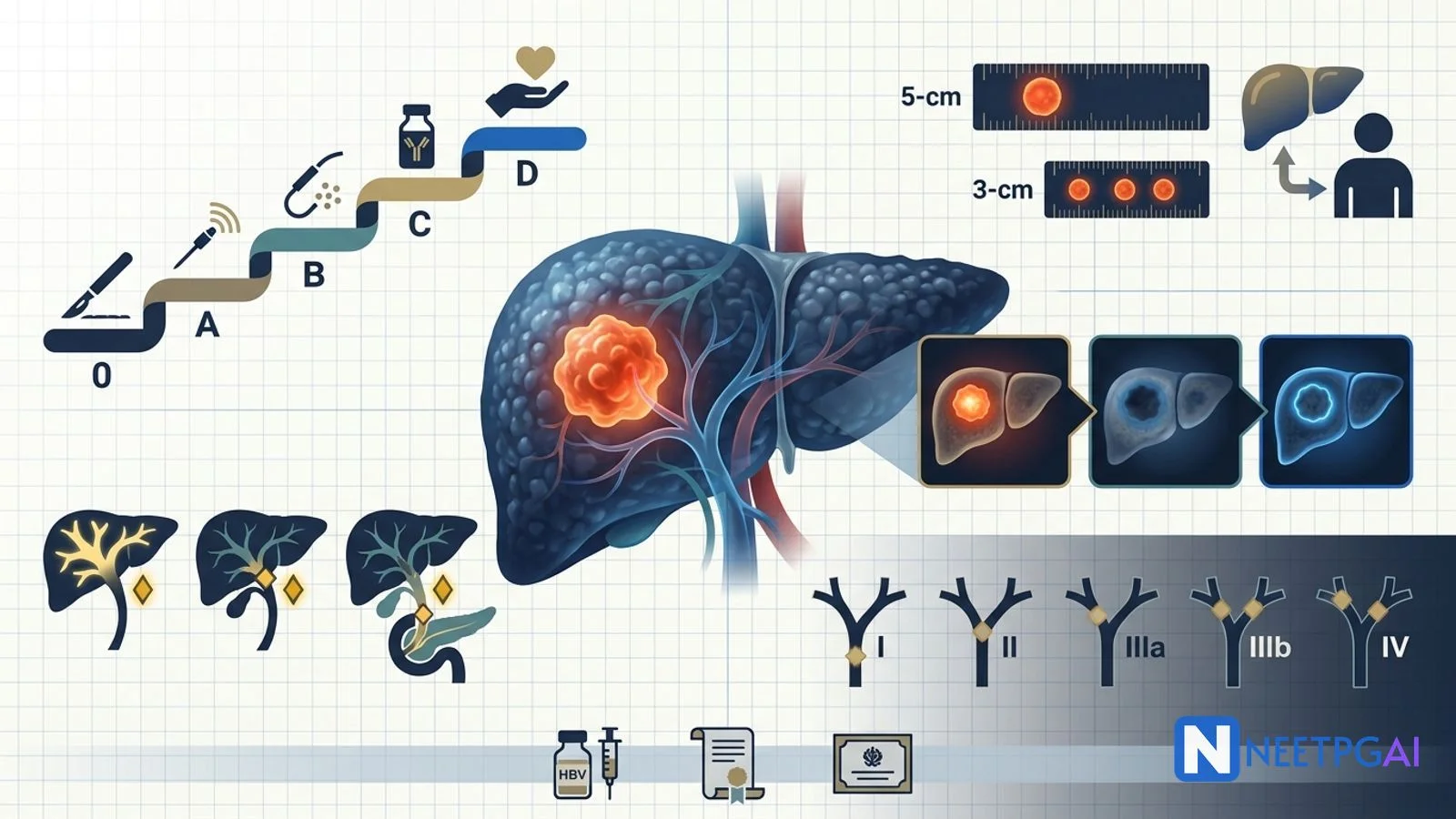
- BCLC staging — 0/A resection or ablation; B → TACE; C → atezolizumab-bevacizumab first-line; D → supportive.
- Milan criteria — one lesion < 5 cm OR up to 3 lesions each < 3 cm; no vascular invasion.
- Cholangiocarcinoma — painless obstructive jaundice; Bismuth-Corlette for perihilar Klatskin tumours.
- India context — HBV birth-dose vaccine (UIP 2011); LTx access limited; NPCDCS covers early detection.
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the third leading cause of cancer death globally. In India, HCC ranks in the top 10 male cancers, driven overwhelmingly by chronic hepatitis B, which affects an estimated 40 million Indians. Cholangiocarcinoma is rarer but similarly lethal, presenting as painless obstructive jaundice with a distinctive Bismuth-Corlette anatomical classification that is a NEET PG staple.
This NEETPGAI deep dive walks through the pathogenesis, LI-RADS non-invasive diagnostic pathway, BCLC staging, Milan criteria for transplant, and the systemic therapy revolution (atezolizumab-bevacizumab and lenvatinib) — plus the cholangiocarcinoma spectrum from intrahepatic to distal. Pair this with the head and neck cancer guide for another oncology-heavy NEET PG staple.
Hepatocellular carcinoma — epidemiology
Global and India context
- Globally — 6th most common cancer; 3rd leading cause of cancer death.
- India — top 10 male cancers; estimated 34,000 new cases per year (GLOBOCAN 2020). Higher incidence in Northeast India and parts of Punjab.
- HBV drives 60 to 70 percent of Indian HCC; HCV and NAFLD are rising.
Risk factors (in decreasing India-specific order)
| Risk factor | Mechanism | India note |
|---|
| Chronic HBV | HBV integration, HBx oncoprotein, chronic inflammation → cirrhosis → HCC | 40 million Indian carriers; birth-dose vaccine in UIP since 2011 |
| Chronic HCV | Cirrhosis-driven; genotype 3 accelerates fibrosis | Falling post-DAA rollout (sofosbuvir + daclatasvir, national programme) |
| NAFLD / MAFLD | Obesity, T2DM, metabolic syndrome → NASH → cirrhosis → HCC | Fastest-rising cause in urban India |
| Alcohol | Cirrhosis; synergistic with HBV/HCV | Especially Kerala, Punjab |
| Aflatoxin B1 | Aspergillus flavus on stored grains; TP53 R249S mutation | Rural India, monsoon-humidity grain storage |
| Haemochromatosis, Wilson disease, α1-antitrypsin, autoimmune hepatitis | Chronic hepatocyte injury | Rare in Indian series |
| Hepatic adenoma | Oral contraceptive use, anabolic steroids | Malignant potential if > 5 cm or β-catenin mutated |
Pathogenesis
- Chronic hepatocyte injury → regeneration → cirrhosis in most cases (except HBV, which can cause HCC without cirrhosis via direct genome integration).
- Dysplastic nodules → early HCC → progressed HCC.
- Key mutations — TERT promoter (60 percent), TP53 (30 percent), CTNNB1 (Wnt/β-catenin, 30 percent).
HCC — screening
Cirrhotic patients (Child-Pugh A/B) and chronic HBV carriers should undergo surveillance every 6 months with:
- Ultrasound of the abdomen — cheap, no radiation; sensitivity 60-70 percent for early HCC.
- Serum alpha-fetoprotein (AFP) — supportive; cutoff 20 ng/mL (some use 200 ng/mL for specificity).
AFP alone is insufficient (false positives in hepatitis flares, pregnancy; false negatives in 30 percent of small HCCs). USG + AFP is the pragmatic Indian standard.
HCC — diagnosis (LI-RADS)
The Liver Imaging Reporting and Data System (LI-RADS) allows non-invasive diagnosis in cirrhotic patients using 4-phase contrast-enhanced CT or MRI.
LI-RADS 5 (definitely HCC) — key features
- Arterial-phase hyper-enhancement (HCC receives dominantly arterial blood).
- Washout on portal-venous or delayed phase (loss of enhancement relative to background).
- Enhancing capsule (fibrous pseudocapsule).
- Size threshold — 10 to 19 mm with growth, or 20 mm or larger.
LI-RADS 5 in a cirrhotic = HCC without biopsy needed.
In non-cirrhotic livers, biopsy is still required (imaging alone insufficient).
Serum markers
- AFP — supportive; over 200 ng/mL in a cirrhotic with LI-RADS 5 is strongly diagnostic.
- AFP-L3 (fucosylated) and DCP / PIVKA-II — improve specificity; used in Japan/Korea, less in India.
HCC — staging (BCLC)
The Barcelona Clinic Liver Cancer (BCLC) system integrates tumour burden, liver function (Child-Pugh) and performance status (ECOG) to assign both stage and stage-directed treatment.
| BCLC | Description | Treatment |
|---|
| 0 — very early | Single lesion < 2 cm; Child-Pugh A; PS 0 | Resection or ablation |
| A — early | Single lesion any size OR up to 3 lesions each <= 3 cm; Child-Pugh A/B; PS 0 | Resection, transplant (Milan), or ablation |
| B — intermediate | Multinodular; preserved function; PS 0 | Transarterial chemoembolisation (TACE) |
| C — advanced | Vascular invasion or extrahepatic spread; PS 1-2 | Systemic — atezolizumab-bevacizumab (1st line); sorafenib, lenvatinib, durvalumab-tremelimumab alternatives |
| D — terminal | Child-Pugh C or PS 3-4 | Best supportive care |
BCLC is updated periodically; the 2022 update established atezolizumab-bevacizumab as first-line for BCLC C after the IMbrave150 trial showed superior OS vs sorafenib (19.2 vs 13.4 months).
HCC — treatment modalities
Curative
- Resection — for single lesions in Child-Pugh A with preserved function and no portal hypertension.
- Liver transplant — ideal for HCC with cirrhosis meeting Milan criteria (one lesion < 5 cm OR up to 3 lesions each < 3 cm; no macrovascular invasion; no extrahepatic spread). 5-year OS over 70 percent.
- Ablation — radiofrequency (RFA) or microwave (MWA) for lesions less than 3 cm; effective alternative to resection.
Locoregional
- TACE (transarterial chemoembolisation) — doxorubicin-loaded microspheres delivered via hepatic artery; standard for BCLC B.
- TARE (radioembolisation) — Y-90 microspheres; alternative to TACE.
Systemic (BCLC C)
| Line | Regimen | Notes |
|---|
| First | Atezolizumab (anti-PD-L1) + bevacizumab (anti-VEGF) | IMbrave150 — best 1st-line OS |
| First (alternative) | Sorafenib (multi-TKI) | Historical standard (SHARP trial); still used if immunotherapy contraindicated |
| First (alternative) | Lenvatinib | Non-inferior to sorafenib |
| First (alternative) | Durvalumab + tremelimumab (HIMALAYA) | Dual-checkpoint |
| Second | Regorafenib, cabozantinib, ramucirumab | Post-sorafenib progressors |
India note — atezolizumab, bevacizumab, lenvatinib and sorafenib are available; access varies with PMJAY panelling. Generic sorafenib remains the most affordable systemic option.
Cholangiocarcinoma
Cholangiocarcinoma arises from bile duct epithelium and is classified anatomically.
Anatomical subtypes
| Subtype | Location | Frequency | Presentation |
|---|
| Intrahepatic | Peripheral intrahepatic ducts | 10-20% | RUQ mass, weight loss (often asymptomatic until advanced) |
| Perihilar (Klatskin) | At confluence of right and left hepatic ducts | 50-60% | Painless obstructive jaundice, pruritus |
| Distal | CBD below cystic duct junction | 20-30% | Painless obstructive jaundice; DDx pancreatic head cancer |
Bismuth-Corlette classification (perihilar)
| Type | Extent |
|---|
| I | Below the confluence — common hepatic duct |
| II | Reaches the confluence but no involvement of secondary radicles |
| IIIa | Involves the right secondary radicles |
| IIIb | Involves the left secondary radicles |
| IV | Multifocal or involves both right and left secondary radicles |
Higher Bismuth type = more complex resection (may need extended hepatectomy + portal vein resection).
Risk factors
- Primary sclerosing cholangitis (PSC) — 10 to 15 percent lifetime risk (highest single risk factor).
- Hepatolithiasis — chronic intrahepatic stones.
- Liver flukes — Clonorchis sinensis, Opisthorchis viverrini (Southeast Asia; low prevalence in India).
- Choledochal cysts — Todani classification; lifelong risk if unresected.
- Chronic HBV and HCV — mainly intrahepatic subtype.
- Thorotrast (historic), primary biliary cholangitis.
Investigations
- MRCP — gold-standard non-invasive imaging; delineates ductal anatomy for Bismuth-Corlette.
- CT — vascular invasion, resectability.
- ERCP with brush cytology — bilateral drainage + tissue for diagnosis.
- CA 19-9 — elevated in 80 percent (false positive in cholangitis, PSC, obstruction; false negative in Lewis-negative individuals — about 10 percent of Indians).
- EUS-FNA — for distal lesions.
Treatment
- Resection with negative margins — the only curative option.
- Intrahepatic — hepatectomy.
- Perihilar — extended hepatectomy + caudate lobectomy + Roux-en-Y hepaticojejunostomy.
- Distal — Whipple pancreaticoduodenectomy.
- Neoadjuvant chemoradiation + transplant — the Mayo protocol for select perihilar cholangiocarcinoma.
- Palliative — biliary stenting (SEMS) for obstructive jaundice, gemcitabine + cisplatin (ABC-02 regimen) as systemic first-line, durvalumab + gem-cis (TOPAZ-1) for advanced disease. FGFR2 fusion inhibitors (pemigatinib, futibatinib) for FGFR2-altered intrahepatic subtype.
Only 20 to 30 percent present with resectable disease; overall 5-year survival remains 5 to 15 percent.
NEET PG MCQ traps
- HBV is the leading cause of HCC in India (60-70 percent) — perinatal transmission drives chronicity.
- HBV can cause HCC without cirrhosis (via genome integration and HBx protein) — unique among hepatitis viruses.
- HCV genotype 3 — most fibrogenic; but DAAs (sofosbuvir + daclatasvir) have national coverage in India.
- Aflatoxin B1 — Aspergillus flavus on stored grains; causes TP53 R249S mutation → HCC.
- HCC surveillance — USG + AFP every 6 months in cirrhotic and chronic HBV.
- LI-RADS 5 = arterial hyper-enhancement + washout + capsule + size threshold → diagnostic without biopsy in cirrhotic.
- AFP — not sensitive alone; over 200 ng/mL + compatible LI-RADS in cirrhotic strongly supports HCC.
- BCLC C first-line — atezolizumab + bevacizumab (IMbrave150).
- Milan criteria — one < 5 cm OR up to 3 lesions each < 3 cm; no vascular invasion; no extrahepatic spread.
- TACE — BCLC B (multinodular, preserved function).
- RFA / MWA — HCC lesions less than 3 cm; alternative to resection.
- Hepatic adenoma — OCP-associated; malignant potential if > 5 cm.
- Cholangiocarcinoma perihilar = Klatskin tumour; most common subtype (50-60 percent).
- Bismuth-Corlette — grades perihilar cholangiocarcinoma extent.
- Klatskin tumour — painless obstructive jaundice; MRCP is gold standard; extended hepatectomy + caudate lobectomy.
- PSC + ulcerative colitis — 10-15 percent lifetime risk of cholangiocarcinoma.
- Liver flukes (Clonorchis, Opisthorchis) — Southeast Asia; not major in India.
- CA 19-9 — false negative in Lewis-negative individuals (about 10 percent of Indians); false positive in cholangitis.
- Distal cholangiocarcinoma — treated with Whipple pancreaticoduodenectomy.
- Gemcitabine + cisplatin (ABC-02) — first-line systemic for unresectable cholangiocarcinoma; durvalumab added (TOPAZ-1) improves OS.
- FGFR2 fusion inhibitors (pemigatinib) — targeted therapy for intrahepatic cholangiocarcinoma with FGFR2 fusions.
Recent updates and India context
- HBV birth-dose vaccination in the Universal Immunisation Programme (UIP) since 2011 — expected to substantially cut HCC incidence in cohorts born after that date. Coverage is now over 80 percent but with state variation.
- NPCDCS (National Programme for Prevention and Control of NCDs including Cancer, Diabetes, CVD, Stroke) — HCC screening in high-risk cirrhotic patients at district hospitals.
- PMJAY / Ayushman Bharat — panelled for liver transplant, sorafenib and locoregional therapy at select tertiary centres.
- NAFLD in urban India — meta-analyses report a 32 percent adult prevalence; NAFLD-HCC is expected to overtake HCV-HCC by 2030.
- Sofosbuvir generic — India's DAA revolution (Cipla, Natco) enabled the National Viral Hepatitis Control Programme (NVHCP), targeting HCV elimination by 2030 with over 95 percent cure rates.
- Liver transplant centres in India — ILBS Delhi, PGIMER Chandigarh, Apollo (Delhi, Chennai, Hyderabad), Medanta Gurgaon, CMC Vellore, Global Hospital (Chennai, Mumbai) do the bulk of adult LTx; annual national volume is about 2,500 (mostly living donor).
- Atezolizumab-bevacizumab — available in India via Roche's PMJAY panel and PharmEasy patient-assistance programmes; average cost 3-4 lakh INR per cycle.
- TARE (Y-90 radioembolisation) — expanding at Tata Memorial (Mumbai), AIIMS (New Delhi), Apollo Delhi and PGIMER Chandigarh.
- AIIMS Delhi HCC guidelines (INASL / Indian National Association for the Study of the Liver) — pragmatic Indian adaptation of BCLC with local cost considerations.
Frequently asked questions
Why is hepatitis B the leading cause of HCC in India?
India has an estimated 40 million chronic HBV carriers, mostly acquired perinatally or in early childhood — routes with the highest chronicity risk (over 90 percent for perinatal vs less than 5 percent for adult acquisition). HBV integrates into the host genome, dysregulates cell cycle genes (via HBx protein), and drives chronic inflammation, cirrhosis and HCC. About 60 to 70 percent of Indian HCC cases are HBV-driven, followed by HCV (with declining incidence post-DAAs), NAFLD, alcohol and aflatoxin exposure. India introduced universal birth-dose hepatitis B vaccination under the Universal Immunisation Programme in 2011, which is expected to substantially reduce HCC incidence in cohorts born after that date.
How can HCC be diagnosed without a biopsy?
In a patient with underlying cirrhosis, HCC can be diagnosed non-invasively using LI-RADS (Liver Imaging Reporting and Data System) criteria on 4-phase contrast-enhanced CT or MRI. A LI-RADS 5 lesion — arterial-phase hyper-enhancement plus washout in the portal-venous or delayed phase plus an enhancing capsule plus a threshold size (10 mm or more, or 10-19 mm with growth) — is diagnostic without biopsy. AFP is a supportive marker but not required; a rising AFP over 200 ng/mL in a cirrhotic with a compatible lesion strongly supports HCC. In non-cirrhotic livers, biopsy is still required.
What is the BCLC staging system and how does it drive treatment?
The Barcelona Clinic Liver Cancer (BCLC) system stages HCC by combining tumour burden, liver function (Child-Pugh) and performance status. Stage 0 (very early) — single lesion less than 2 cm, Child-Pugh A → resection or ablation. Stage A (early) — single lesion or up to 3 lesions each 3 cm or less → resection, transplant (Milan criteria) or ablation. Stage B (intermediate) — multinodular but preserved function → TACE. Stage C (advanced) — vascular invasion or extrahepatic spread → systemic therapy (atezolizumab-bevacizumab first-line, sorafenib or lenvatinib alternatives). Stage D (terminal) — Child-Pugh C or PS 3-4 → best supportive care. BCLC is updated periodically; the 2022 update added atezolizumab-bevacizumab as first-line for advanced disease.
What are the Milan criteria for liver transplant in HCC?
The Milan criteria (Mazzaferro, 1996) select HCC patients for liver transplantation with acceptable long-term outcomes — one lesion less than 5 cm, or up to 3 lesions each less than 3 cm, with no macrovascular invasion and no extrahepatic spread. Patients meeting Milan achieve 5-year survival over 70 percent post-transplant, comparable to non-HCC indications. Expanded criteria (UCSF, Up-to-7) allow larger tumours if biology is favourable, and downstaging via TACE or ablation to bring tumours within Milan is standard practice at Indian tertiary centres like ILBS Delhi, PGIMER Chandigarh, Apollo, Medanta and CMC Vellore.
Why is cholangiocarcinoma associated with painless obstructive jaundice?
Cholangiocarcinoma arises from bile duct epithelium and, depending on location, obstructs bile flow. Perihilar (Klatskin) tumours at the confluence of the right and left hepatic ducts and distal common bile duct tumours cause painless progressive jaundice, pale stools, dark urine, pruritus and weight loss — the classic 'obstructive' presentation. Unlike gallstones (which cause colicky pain), malignant obstruction is often painless. The Bismuth-Corlette classification (I through IV) grades perihilar involvement of hepatic ducts and dictates resection complexity. MRCP is the imaging of choice; CA 19-9 elevation supports diagnosis. Resection with negative margins is the only curative option; only about 20 to 30 percent of patients present with resectable disease.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: July 2026