Version 1.0 — Published April 2026
Quick Answer
Non-contrast CT is the first-line imaging modality in suspected stroke — it distinguishes ischemic from hemorrhagic stroke within minutes, driving immediate treatment decisions (thrombolysis, thrombectomy, or neurosurgical referral). To correctly interpret CT brain stroke MCQs in NEET PG, follow this 5-step approach:
- Check symmetry — compare both hemispheres at matched axial levels for sulcal effacement, gray-white loss, or focal hypodensity
- Look for the hyperdense MCA sign — focal hyperdensity (77-89 HU) within the proximal MCA indicates acute thrombus; earliest CT sign of stroke
- Assess cisterns and ventricles — effaced basal cisterns suggest raised ICP or herniation; intraventricular blood is a grave prognostic sign in ICH
- Score using ASPECTS for MCA territory — 10 regions, 1 point deducted per ischemic region; score 6 or above supports thrombolysis or thrombectomy
- Identify hemorrhage pattern — ICH (rounded, parenchymal, basal ganglia in hypertensives), SAH (cisternal, aneurysmal), SDH (crescent, crosses sutures), EDH (biconvex, does NOT cross sutures)
Clinical image presentation
A 72-year-old right-handed man with a history of atrial fibrillation (not on anticoagulation due to a fall 6 months ago) is brought to the emergency department at 9:15 AM. His wife reports that he woke at 7:00 AM, was normal at breakfast, then slumped over the newspaper at 8:30 AM. She found him with right-sided weakness and slurred speech.
On arrival, his NIHSS score is 14. He has right facial droop, right hemiplegia (grade 2/5 upper limb, 3/5 lower limb), expressive aphasia, and right homonymous hemianopia. BP is 168/96 mmHg, glucose 112 mg/dL, temperature 98 F. The last known well time is 8:15 AM — 60 minutes before presentation.
A non-contrast CT brain is performed immediately. A student should systematically identify these findings:
Level 1 — basal ganglia (third ventricle visible):
- Focal hyperdensity within the left M1 segment of the middle cerebral artery (density approximately 85 Hounsfield units) — the hyperdense MCA sign
- Subtle loss of gray-white matter differentiation in the left insular cortex — insular ribbon sign
- Obscuration of the left lentiform nucleus (normal gray matter density diminished)
- Early sulcal effacement over the left hemisphere
Level 2 — supraganglionic slices:
- No established hypodensity yet (consistent with hyperacute ischemia within 3-4 hours of onset)
- No hemorrhage in any compartment
- No midline shift, ventricles symmetric, cisterns patent
- No intraventricular blood
Bone windows:
- No skull fracture
- No extracranial hematoma
MCQ question as it appears in NEET PG
A 72-year-old man with atrial fibrillation presents 60 minutes after the onset of right hemiplegia and expressive aphasia. Non-contrast CT brain shows focal hyperdensity within the left proximal middle cerebral artery measuring approximately 85 Hounsfield units, with subtle obscuration of the left insular ribbon and lentiform nucleus. No hemorrhage. Which of the following is the most appropriate next step?
- (a) Start IV alteplase immediately after confirming no contraindications
- (b) Order MRI brain to confirm infarct before treatment
- (c) Start dual antiplatelet therapy with aspirin plus clopidogrel
- (d) Wait and repeat CT in 6 hours
Take a moment to work through this before reading the analysis below.
Step-by-step visual analysis
A systematic reading protocol is critical — missing the hyperdense MCA sign or insular ribbon sign means missing the earliest indicators of large-vessel occlusion and losing the thrombolysis window. Use this protocol every time a CT brain appears in an NEET PG stroke MCQ.
Step 1: Confirm technical adequacy and orientation
- Is the scan complete? Axial slices from foramen magnum to vertex.
- Is the head symmetric? Tilted scans produce pseudo-asymmetry. Mentally rotate if needed.
- What is the window? Default brain window (WW 80, WL 40) shows parenchyma. Bone window (WW 2000, WL 400) shows fractures. Subdural window (WW 200, WL 70) highlights thin extra-axial blood.
Step 2: Check symmetry of the hemispheres
Compare both hemispheres at matched axial levels:
- Sulci — are they equally prominent? Unilateral effacement is an early stroke sign.
- Gyri — is the gray-matter ribbon visible symmetrically?
- Density — are the deep gray structures (caudate, lentiform, thalamus) equally dense on both sides? A hypodense caudate or lentiform is an early ischemic sign.
- Midline structures — is the falx in the midline? Shift suggests mass effect from stroke edema or hemorrhage.
Step 3: Look for hyperdense vessel signs
Hyperdense artery signs are the earliest CT findings in ischemic stroke — they reflect intraluminal thrombus, not parenchymal damage.
- Hyperdense MCA sign — focal hyperdensity along the course of the M1 or M2 segment (density 77-89 HU; normal unclotted blood is 35-60 HU). Sensitivity 30-50 percent, specificity above 90 percent. Strongly suggests large-vessel occlusion.
- MCA dot sign — hyperdensity in the M2 or M3 sylvian branches.
- Hyperdense basilar artery — similar finding in posterior circulation stroke (carries a grave prognosis).
- Hyperdense internal carotid artery — indicates terminal ICA thrombus ("T-lesion") with poor collateral supply.
Step 4: Identify early ischemic changes
Early ischemic changes appear as subtle parenchymal findings within 3-6 hours:
- Loss of gray-white matter differentiation — the earliest parenchymal sign; normal cortical gray matter is slightly denser than white matter.
- Insular ribbon sign — loss of the normal ribbon of gray matter in the insular cortex.
- Obscuration of the lentiform nucleus — the putamen and globus pallidus become less distinct from surrounding white matter.
- Cortical sulcal effacement — subtle compression of sulci from cytotoxic edema.
- Dense deep nuclei — the caudate or lentiform may look denser than the opposite side when adjacent white matter becomes edematous.
In this patient: all four features are present in the left MCA territory — consistent with hyperacute MCA occlusion.
Step 5: Score using ASPECTS (for MCA territory infarcts)
ASPECTS is a reproducible 10-point system for MCA territory infarcts on non-contrast CT:
- Basal ganglia level (5 regions): caudate, lentiform, internal capsule, insular ribbon, M1 (anterior MCA cortex), M2 (MCA cortex lateral to insular ribbon), M3 (posterior MCA cortex).
- Supraganglionic level (3 regions): M4 (anterior), M5 (lateral), M6 (posterior) MCA cortex.
- Scoring: start at 10. Subtract 1 for each region showing early ischemic change.
ASPECTS 6 or above supports IV thrombolysis and mechanical thrombectomy. ASPECTS below 6 indicates a large established infarct with higher risk of hemorrhagic transformation.
In this patient: ASPECTS is approximately 7 (insular ribbon, lentiform, and M1 cortex affected).
Step 6: Exclude hemorrhage in every compartment
Hemorrhage must be actively excluded before any antithrombotic therapy:
- Intracerebral (ICH) — rounded hyperdensity in brain parenchyma, 60-80 HU acutely
- Subarachnoid (SAH) — hyperdensity in sulci, basal cisterns, sylvian fissures, interhemispheric fissure
- Subdural (SDH) — crescent-shaped extra-axial collection, crosses suture lines
- Epidural (EDH) — biconvex (lens-shaped) extra-axial collection, does NOT cross suture lines
- Intraventricular — hyperdense layered blood in lateral or third ventricles
In this patient: no hemorrhage in any compartment — ischemic etiology confirmed.
Answer and detailed explanation
Correct answer: (a) Start IV alteplase immediately after confirming no contraindications
This patient has acute ischemic stroke within the 4.5-hour alteplase window (60 minutes from last known well) with no hemorrhage and no visible large established hypodensity on CT. The hyperdense MCA sign with ASPECTS 7 is fully consistent with hyperacute ischemia amenable to thrombolysis. IV alteplase (0.9 mg/kg, 10 percent as bolus over 1 minute, remaining 90 percent as infusion over 60 minutes; maximum 90 mg) is indicated per 2019 AHA/ASA guidelines after confirming absence of contraindications (BP controlled below 185/110, no recent bleeding, platelets above 100,000, INR below 1.7, no major surgery in past 2 weeks).
Because the hyperdense MCA sign and clinical NIHSS of 14 suggest large-vessel occlusion, CT angiography should be obtained urgently to confirm M1 occlusion and refer for mechanical thrombectomy — the DAWN and DEFUSE 3 trials (NEJM, 2018) extended the thrombectomy window to 24 hours for selected patients with small core and large penumbra.
Why each distractor is wrong:
| Option | Why incorrect |
|---|
| (b) Order MRI to confirm | MRI provides higher sensitivity for hyperacute ischemia but is NOT required before thrombolysis when CT shows no hemorrhage. Delaying treatment for MRI wastes the narrow 4.5-hour window. "Time is brain" — 1.9 million neurons die per minute of untreated large-vessel occlusion. |
| (c) Start DAPT (aspirin + clopidogrel) | DAPT is the treatment for minor ischemic stroke or high-risk TIA (NIHSS 3 or below, from CHANCE and POINT trials) — not major acute stroke within the thrombolysis window. Antiplatelet therapy is started 24 hours AFTER thrombolysis, not instead of it. |
| (d) Wait and repeat CT | Waiting wastes the therapeutic window. Thrombolysis must be given within 4.5 hours of last known well, and mechanical thrombectomy within 6-24 hours depending on perfusion imaging. |
NEET PG trap alert: The most common wrong answer chosen is MRI confirmation. Remember: a non-contrast CT that excludes hemorrhage is sufficient to start IV alteplase in eligible patients. MRI is used when CT is inconclusive or for posterior circulation stroke where CT sensitivity is lower.
Practice neurology MCQs with AI-powered explanations to build stroke pattern recognition. For a full review, see our comprehensive stroke management guide and build medicine subject coverage with targeted drills.
Similar patterns comparison table
The five CT patterns most commonly tested in NEET PG stroke image MCQs — memorize this table, it covers approximately 85 percent of stroke imaging questions:
| CT finding | Diagnosis | Key distinguishing features |
|---|
| Hyperdense MCA sign + subtle gray-white loss + normal density of surrounding tissue | Hyperacute ischemic stroke (0-6 hours) | Focal vessel hyperdensity, ASPECTS usually 7-10, treatment window open for thrombolysis and thrombectomy |
| Wedge-shaped hypodensity in MCA territory + sulcal effacement + preserved deep gray | Acute ischemic stroke (6-24 hours) | Established parenchymal changes, ASPECTS variable, window closed for thrombolysis but thrombectomy possible up to 24 hours with favorable perfusion |
| Rounded hyperdense mass in basal ganglia (putamen most common) with surrounding hypodense edema | Hypertensive intracerebral hemorrhage | Middle-aged or elderly hypertensive patient, often with intraventricular extension, surgical evacuation controversial (STICH II trial) |
| Hyperdensity in basal cisterns, sylvian fissure, interhemispheric fissure | Subarachnoid hemorrhage | Thunderclap headache, aneurysmal in 85 percent (circle of Willis), CT sensitivity highest in first 6 hours, lumbar puncture if CT negative |
| Crescent-shaped hyperdensity along convexity, crosses suture lines, may span entire hemisphere | Acute subdural hematoma | Elderly with fall, anticoagulated patients; from bridging vein tear; chronic SDH is isodense or hypodense |
| Biconvex (lens-shaped) hyperdensity, limited by suture lines, typically temporal | Epidural hematoma | Trauma with middle meningeal artery injury; classic "lucid interval" between injury and deterioration; neurosurgical emergency |
| Hypodense wedge-shaped territorial infarct with evolving gyral enhancement on contrast | Subacute ischemic stroke (1-2 weeks) | Peak edema at 3-5 days, gyral enhancement from blood-brain barrier breakdown, may show hemorrhagic transformation |
| Hypodense MCA territory with ex vacuo dilation of adjacent ventricle | Chronic ischemic stroke (weeks-months) | Gliosis, encephalomalacia, negative mass effect with compensatory ventricular enlargement |
| Hyperdense rim around hypodense collection | Cerebral abscess (ring-enhancing on contrast) | Fever, immunosuppression, adjacent sinus infection; distinguished from tumor by DWI restriction |
| Hyperdensity along the superior sagittal sinus ("dense triangle sign") | Cerebral venous sinus thrombosis | Young woman on OCPs, postpartum, or with thrombophilia; MR venography is confirmatory |
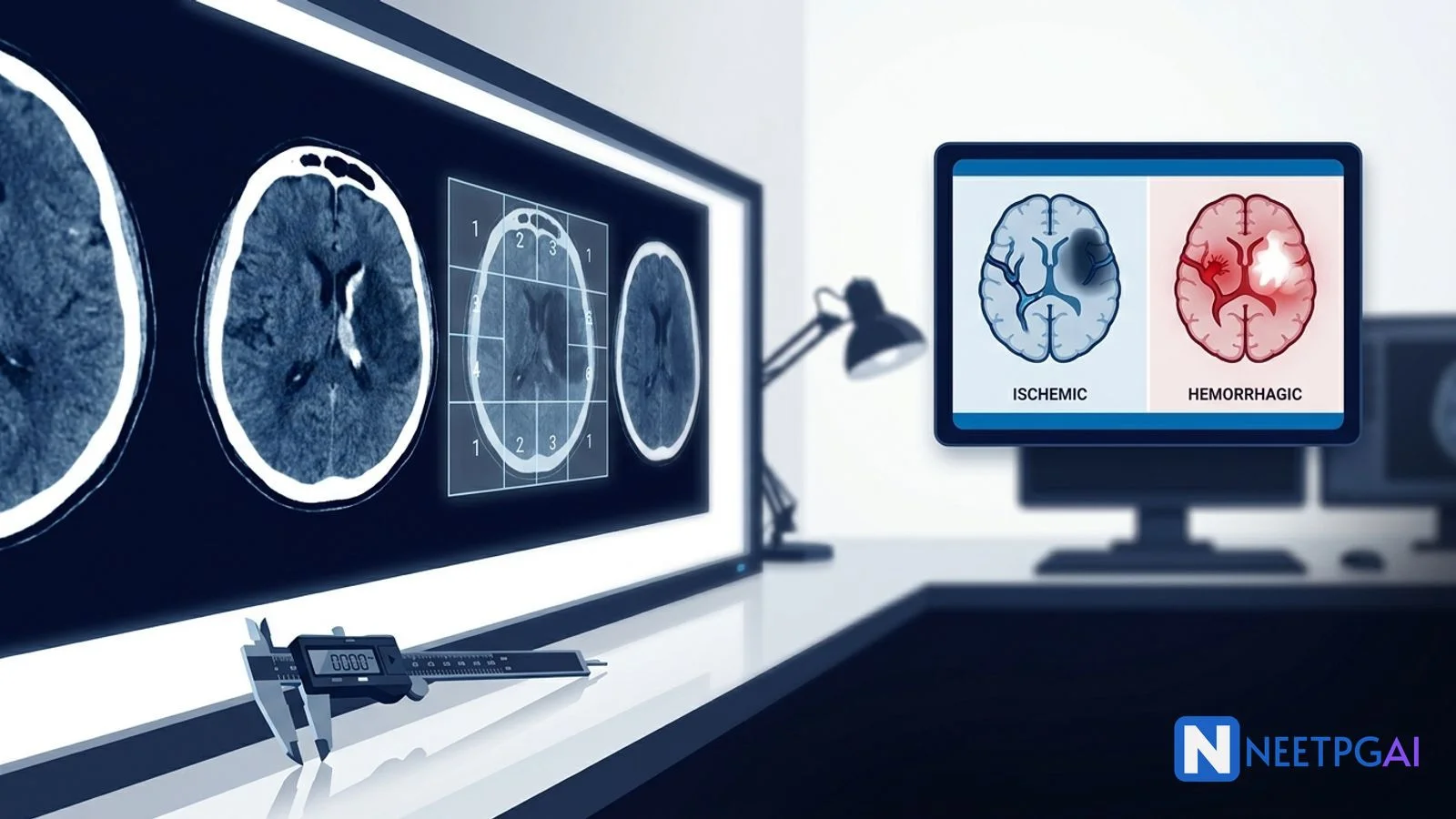
Clinical application: differentiating ischemic from hemorrhagic stroke
Non-contrast CT is the first study in every suspected stroke because the management diverges completely based on hemorrhage vs ischemia — thrombolysis saves lives in ischemic stroke and kills patients with hemorrhagic stroke.
The key discriminators at a glance:
| Feature | Ischemic stroke | Hemorrhagic stroke (ICH) |
|---|
| CT appearance (acute) | Normal or subtle hypodensity; hyperdense vessel sign | Rounded hyperdense parenchymal mass (60-80 HU) |
| Common location | MCA territory (cortical wedge); lacunes in deep gray | Basal ganglia (putamen), thalamus, pons, cerebellum |
| Typical onset | Focal deficit at waking or during activity | Severe headache, vomiting, rapid deterioration |
| Precipitating factors | Atrial fibrillation, carotid disease, atherosclerosis | Uncontrolled hypertension, amyloid angiopathy, anticoagulation |
| Initial BP management | Permissive hypertension up to 220/120 (before lysis) or 185/110 (for lysis) | Aggressive lowering to SBP 140 (INTERACT2, NEJM 2013) |
| Antithrombotic therapy | Antiplatelet within 24-48 hours; anticoagulation depends on etiology | Contraindicated; reverse anticoagulation urgently |
| Surgical role | Thrombectomy if large-vessel occlusion | Hematoma evacuation selectively (cerebellar above 3 cm, superficial lobar) |
Cerebellar hemorrhage above 3 cm diameter, any cerebellar hemorrhage with brainstem compression or hydrocephalus, and superficial lobar hematomas in deteriorating patients warrant urgent neurosurgical evacuation. Deep hemorrhages (basal ganglia, thalamus) generally do not benefit from surgery per the STICH II trial (Lancet, 2013).
Frequently asked questions
What is the systematic approach to reading a CT brain in a suspected stroke?
Use the symmetry-cisterns-ventricles-gray-white-bone (SCVGB) protocol. First, check symmetry of both hemispheres at matched levels — any asymmetry of sulci, gyri, or density suggests pathology. Second, examine basal cisterns (suprasellar, ambient, quadrigeminal) — effacement suggests raised ICP or herniation. Third, check ventricles for size, shift, or intraventricular blood. Fourth, assess gray-white matter differentiation — loss is the earliest sign of ischemic infarct. Fifth, review bone windows for fractures. This 5-step approach prevents missing subtle early ischemic signs and hyperdense vessel signs.
What is the hyperdense MCA sign and when is it seen?
The hyperdense middle cerebral artery (MCA) sign is a focal hyperdensity (density 77-89 Hounsfield units) within the course of the proximal MCA on non-contrast CT, representing an acute thrombus within the vessel lumen. It is visible within minutes of occlusion, before any parenchymal changes develop. Sensitivity is 30-50 percent, specificity above 90 percent. A related sign is the MCA dot sign — hyperdensity in the M2 or M3 sylvian branches. Both strongly suggest large-vessel occlusion amenable to mechanical thrombectomy.
How do early ischemic changes evolve on CT over the first 24 hours?
CT changes follow a predictable timeline. Hyperacute (0-6 hours) — hyperdense MCA sign, subtle loss of gray-white differentiation, insular ribbon sign, obscuration of the lentiform nucleus, cortical sulcal effacement. Acute (6-24 hours) — overt hypodensity appears in the infarcted territory, mass effect develops. Subacute (24 hours-1 week) — progressive hypodensity with wedge-shaped cortical involvement, peak edema at 3-5 days. CT is relatively insensitive for hyperacute ischemia — MRI with diffusion-weighted imaging (DWI) detects infarct within minutes.
What is ASPECTS and how is it calculated?
ASPECTS (Alberta Stroke Program Early CT Score) is a 10-point scoring system for MCA territory infarcts on non-contrast CT. The MCA territory is divided into 10 regions: caudate, lentiform nucleus, internal capsule, insular ribbon, and M1-M6 cortical regions (M1-M3 at basal ganglia level, M4-M6 at supraganglionic level). Each region showing early ischemic change (hypodensity or gray-white loss) deducts 1 point. Normal CT scores 10; total MCA infarct scores 0. ASPECTS 6 or above supports thrombolysis or thrombectomy; ASPECTS below 6 suggests large established infarct with higher risk of hemorrhagic transformation.
How do you distinguish intracerebral hemorrhage from subarachnoid, subdural, and epidural bleeds on CT?
Location and shape are the key features. Intracerebral hemorrhage (ICH) — rounded or lobular hyperdensity within brain parenchyma, common in basal ganglia (hypertensive). Subarachnoid hemorrhage (SAH) — hyperdensity in basal cisterns, sylvian fissures, and sulci, often aneurysmal. Subdural hematoma (SDH) — crescent-shaped collection crossing suture lines, from bridging vein tear. Epidural hematoma (EDH) — biconvex (lens-shaped) collection that does NOT cross suture lines, from middle meningeal artery tear. Acute blood is hyperdense (60-80 HU); subacute (1-2 weeks) is isodense; chronic (above 2 weeks) is hypodense.
What is the role of CT perfusion and CT angiography in acute stroke?
CT angiography (CTA) identifies large-vessel occlusion candidates for mechanical thrombectomy — typically ICA, M1, M2, or basilar artery occlusion. CT perfusion (CTP) distinguishes infarct core (matched defect on cerebral blood flow and blood volume) from penumbra (blood flow reduced but blood volume preserved — salvageable tissue). The DEFUSE 3 and DAWN trials (NEJM, 2018) established that patients with small core and large penumbra benefit from thrombectomy up to 16-24 hours from onset, extending the treatment window dramatically.
What are the contraindications to IV thrombolysis with alteplase in acute ischemic stroke?
Absolute contraindications include active bleeding or high bleeding risk, recent intracranial hemorrhage, ischemic stroke within 3 months, intracranial or intraspinal surgery in past 3 months, head trauma in past 3 months, suspected SAH, platelets below 100,000, INR above 1.7, heparin within 48 hours with elevated aPTT, and BP above 185/110 that cannot be controlled. Relative contraindications include major surgery in past 2 weeks, GI bleeding in past 3 weeks, pregnancy, seizure at stroke onset with postictal deficit, and minor or rapidly improving symptoms. The window is 4.5 hours from symptom onset for IV alteplase.
How is CT brain tested in NEET PG?
NBE tests CT brain interpretation through four patterns: identifying the hyperdense MCA sign (earliest CT sign of ischemic stroke), distinguishing infarct from the five hemorrhage types (ICH, SAH, SDH, EDH, intraventricular) by location and shape, recognizing early ischemic changes (loss of gray-white differentiation, insular ribbon sign, sulcal effacement), and choosing appropriate next steps (thrombolysis window, thrombectomy criteria, ASPECTS cutoff). Expect 1-2 CT brain questions per NEET PG paper across medicine, radiology, and neurology sections.
This content is for educational purposes for NEET PG exam preparation. It is not a substitute for professional medical advice, diagnosis, or treatment. Clinical information has been reviewed by qualified medical professionals.
Sources and references
- Osborn's Brain: Imaging, Pathology, and Anatomy, 3rd Edition (Osborn et al., 2020) — comprehensive neuroradiology reference for CT and MRI interpretation of stroke and hemorrhage.
- Powers WJ et al., "Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update," Stroke, 2019 — AHA/ASA guideline for thrombolysis, thrombectomy indications, and imaging criteria.
- Nogueira RG et al., "Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct (DAWN trial)," New England Journal of Medicine, 2018 — landmark trial extending the thrombectomy window using CT perfusion imaging.
Strengthen your stroke pattern recognition by working through neuroimaging vignettes. Review the comprehensive stroke management guide, build your medicine subject coverage, and drill targeted CT brain questions on the NEETPGAI practice platform. Ready for unlimited AI-powered MCQs with detailed explanations? Explore NEETPGAI Pro.
For personalized study guidance on radiology and neurology, try the AI Tutor — it adapts to your weak areas and explains concepts the way a senior resident would.
Written by: NEETPGAI Editorial Team
Reviewed by: Pending SME Review
Last reviewed: April 2026
This article is reviewed by qualified medical professionals for clinical accuracy and exam relevance. For corrections or updates, contact the editorial team.